Prostate cancer is one of the most common new cancer diagnosed in the USA every year,
and is the cause of around 10% of cancer-related mortality in American men.
In our country,
Colombia,
prostate cancer is considered the second cause of cancer-related deaths in men,
and takes the first place on incidence (Fig. 2).
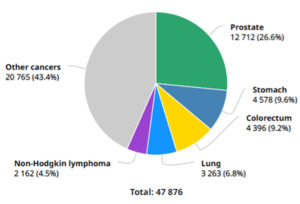
Fig. 2: Globocan 2018 – Colombia. Number of new diagnosed cancer cases in males in 2018, all ages.
References: New Global Cancer Data: GLOBOCAN 2018
There has been a high evidence of over diagnosis and over treatment throughout decades,
even more in low risk patients.
There is also a great variability in its detection,
including different modalities,
for instance,
the digital rectal exam (DRE),
quantification of serum prostatic specific antigen (PSA) and ultrasound guided biopsy.
Which means it is difficult to objectify the neoplastic disease,
its location,
compromise and the whole extension.
The identification of prostate cancer mimickers is important for an adequate interpretation of MR images,
due to its increased role in the diagnostic workup of prostate cancer patients.
There is a wide spectrum of entities,
both anatomic and pathologic,
that may mimic and masquerade as prostate cancer,
making difficult the imaging interpretation (Fig. 3).
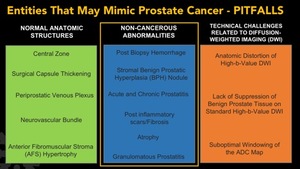
Fig. 3: Entities that may mimic or masquerade as prostate cancer, better known as PITFALLS.
Some anatomical structures can simulate cancer,
such as: central zone,
thickening of the surgical capsule,
the periprostatic venous plexus,
the neurovascular bundle and also the anterior fibromuscular stroma hypertrophy.
There are also some technique aspects related to the acquisition of DW images that can be confounded with malignancy,
such as,
anatomic distortion of high b-value DWI,
the lack of suppression of benign prostate tissue on standard high b-value DWI and a suboptimal windowing of the ADC map.
Furthermore,
there are also some non-cancerous conditions that may masquerade as prostate cancer,
which include,
both acute and chronic prostatitis as important mimickers of prostate cancer,
areas of atrophy or scaring,
benign prostatic hyperplasia,
post biopsy hemorrhage and granulomatous prostatitis.
In this exhibit,
we will review the vast majority of non-neoplastic abnormalities that may simulate tumors,
with special emphasis on granulomatous prostatitis (GP).
GP is a benign inflammatory process rarely encountered in clinical practice,
mainly affecting men in their sixth to eighth decades,
and is classified into nonspecific (idiopathic),
specific (infectious),
iatrogenic (postsurgery),
malacoplakia and is rarely associated with systemic causes.
MR Imaging manifestations of GP are reviewed based on several cases,
focusing on multiparametric studies.
Normal Anatomy of the Prostate Gland
The prostate is an exocrine gland part of the male reproductive system,
which is located between the bladder and the penis,
just in front of the rectum.
The main function of this gland is to secrete an alkaline fluid that nourishes and protects sperm,
and it represents around 30-35% of the human semen.
The gland is limited by a capsule,
known as the prostatic capsule.
When addressing the prostate it is also important to mention the seminal vesicles.
The seminal vesicles are a pair of tubular glands which are localized posterior and inferior to the urinary bladder.
They are in charge of secretion of a significant proportion of the fluid that becomes semen.
The prostate also produces a protein called “Prostatic Specific Antigen”,
better known as PSA.
This protein is measure in blood serum and it can be elevated in some benign or malignant conditions of the gland.
Anatomically,
the gland is divided into zones and lobes.
Zones were first used in pathology,
however,
nowadays,
they are widely used in diagnostic images.
The prostate has four different zones:
- Peripheral zone (PZ),
which accounts for about the 70% of the whole gland.
- Central zone (CZ),
which is approximately 25%.
- Transitional zone (TZ) and,
- Anterior fibromuscular stroma (AFS).
The gland is also divided into lobes,
which include:
- Anterior
- Posterior
- Right and left lateral
- Middle
For the interpretation of diagnostic images of the prostate,
and a proper surgical or pre-biopsy planning,
it is currently being used the anatomic segmentation proposed by the latest “Prostate Imaging Reporting and Data System” version (PI-RADS v2).
This anatomical segmentation model consists of 39 regions,
which include 36 for the prostate,
the two seminal vesicles and the external urethral sphincter.
It also proposes a sector map for using on reporting (Fig. 4).
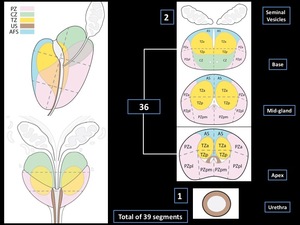
Fig. 4: Adapted from the prostate segmentation model proposed by PI-RADS v2.
References: American College of Radiology © copyright 2015. Prostate Imaging – Reporting and Data System (PI-RADS ™) . Version 2.
It is so important to learn how to recognize each of the zones and segments said above in the interpretation of MR imaging (Fig. 5, Fig. 6,
Fig. 7,
Fig. 8).
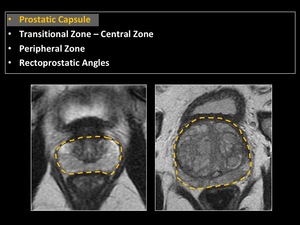
Fig. 5: Anatomy of the prostate gland. Prostatic capsule.
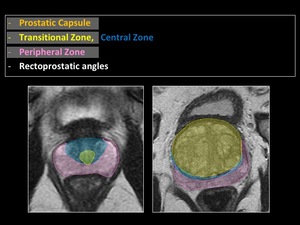
Fig. 6: Anatomy of the prostate gland. Zones.
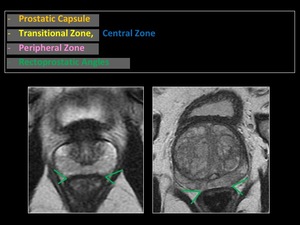
Fig. 7: Anatomy of the prostate gland. Rectoprostatic angles.
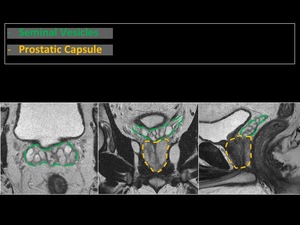
Fig. 8: Anatomy of the prostate gland. Seminal vesicles and prostatic capsule.
Multiparametric Prostate MR Imaging Protocol (MP-MR)
At our institution,
MP-MR imaging is routinely performed at a 3 Tesla magnet,
using Multi-channel surface array and integrated spine coils and it takes around 30 to 45 minutes to performed the whole exam.
The Prostate MP-MR mandatory includes multiplanar T2 Weighted Images (T2WI) in three different planes (Axial,
Sagittal and Coronal + Axial Fat Sat),
T1 Weighted Images (T1WI) in one plane (Axial + Axial Fat Sat),
Dynamic Contrast Enhanced Images (DCE) (0,2 ml/kg of contrast),
and Diffusion Weighted Images (DWI) with a b value of at least 1400 s/mm2 with its Apparent Diffusion Coefficient (ADC) map.
(Fig. 9).
Nowadays,
our protocol has started to included some fusion images of T2WI+DWI and permeability (Fig. 10).
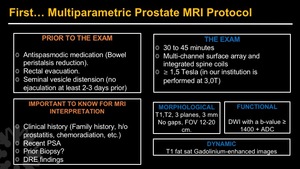
Fig. 9: Prostate MP-MR – Protocol.
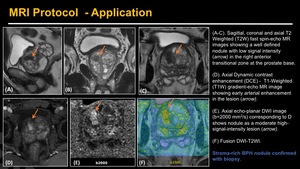
Fig. 10: Prostate MP-MR – Protocol - Application.
(A-C). Sagittal, coronal and axial T2 Weighted (T2W) fast spin-echo MR images showing a well defined nodule with low signal intensity (arrow) in the right anterior transitional zone at the prostate base.
(D). Axial Dynamic contrast enhancement (DCE) - T1-Weighted (T1W) gradient-echo MR image showing early arterial enhancement in the lesion (arrow).
(E). Axial echo-planar DWI image (b=2000 mm2/s) corresponding to D shows nodule as a moderate high-signal-intensity lesion (arrow).
(F) Fusion DWI-T2WI.
Prior to the MR examination we suggest to take an oral antispasmodic drug in order to reduce bowel movements and also to reduce artifacts in the image.
The patient is also asked to do rectal evacuation juts before starting the examination.
The seminal vesicles have to be distended for the day of the examination (no ejaculation at least 2-3 days prior).
For the interpretation of the MR,
it is very important to know the patient’s clinical history,
including some serological data,
among which are:
- Familial history of prostate cancer or any other condition with the gland.
- Personal history of prostatitis,
chemo or radiotherapy,
any medications.
- A recent serum PSA.
- If the patient have had a prior biopsy.
- DRE findings.



 . Version 2.")





. Sagittal, coronal and axial T2 Weighted (T2W) fast spin-echo MR images showing a well defined nodule with low signal intensity (arrow) in the right anterior transitional zone at the prostate base.
(D). Axial Dynamic contrast enhancement (DCE) - T1-Weighted (T1W) gradient-echo MR image showing early arterial enhancement in the lesion (arrow).
(E). Axial echo-planar DWI image (b=2000 mm2/s) corresponding to D shows nodule as a moderate high-signal-intensity lesion (arrow).
(F) Fusion DWI-T2WI.")