NORMAL ANATOMIC STRUCTURES
- Central zone
- Surgical capsule thickening
- Periprostatic venous plexus
- Neurovascular bundle
- Anterior fibromuscular stroma (AFS) hypertrophy
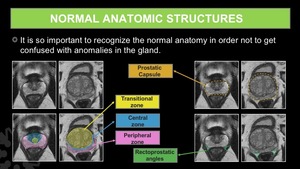
Fig. 11: Normal anatomic structures of the prostate gland.
Central zone (CZ)
- The CZ is a symmetric band localized between the PZ and TZ at the base of the prostate,
which surrounds the ejaculatory ducts and goes from below the seminal vesicles to the verumontanum.
- MR Findings: homogeneous low signal on T2WI with decreased ADC value in relation to the PZ.
On DCE,
the CZ can show a progressive (type 1) or an early enhancement and plateau (type 2) curve.
- When the CZ looks asymmetric or the TZ is enlarged and comprises the CZ,
It can mimic prostate cancer.
Prostate cancer tends to have an early enhancement and washout (type 3 curve)
Surgical Capsule Thickening
- The surgical capsule has been described as a band of fibromuscular tissue which demarcates the TZ,
at the junction of the TZ and PZ.
This capsule makes part of the supporting network of the prostate.
- MR Findings: thin band with low signal on T2WI and ADC map,
surrounding the TZ.
- When the capsule is thickened or appears asymmetric,
it may masquerade as a prostate cancer in a linear fashion,
rather than as a confined mass.
Periprostatic Venous Plexus (PVP)
- The PVP is made of the normal prostatic veins and goes by the lateral and anterior margins of the prostate gland to finally drain into the iliac veins.
- MR Findings: tubular structures with high signal on T2WI.
- This veins can appear of low signal intensity in T2WI and ADC maps,
if there is turbulence or depending on the velocity.
They can also look crowded and prominent,
which mixed with the low signal on T2WI and ADC maps,
can simulate an intraprostatic lesion.
Neurovascular Bundle
- Cavernous neural plexus located near the prostate which gives rise to nervous branches that supply the corpora cavernosa.
This plexus is in strict relation to some arteries,
veins and other nerves,
together forming the whole neurovascular bundle.
- It goes by the posterior and lateral margins of the prostate gland.
- MRI Findings: rounded appearance on axial plane with low signal on T2WI and signal void on ADC maps.
- In some cases,
it looks like located within the PZ on ADC maps causing some anatomical distortion which can lead to a confussion with a mass lesion.
Anterior Fibromuscular Stroma (AFS) Hypertrophy
- AFS is a band of fibromuscular tissue located anteriorly to the TZ.
- MRI Findings: markedly low signal on T2WI and low signal on ADC maps.
- The AFS is supposed to be midline and symmetric.
However,
it could be sometimes,
prominent and bulky,
mimicking prostate cancer (Fig. 12).
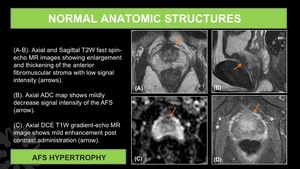
Fig. 12: AFS Hypertrophy.
(A-B). Axial and Sagittal T2W fast spin-echo MR images showing enlargement and thickening of the anterior fibromuscular stroma with low signal intensity (arrows).
(C). Axial ADC map shows mildly decrease signal intensity of the AFS (arrow).
(D). Axial DCE T1W gradient-echo MR image shows mild enhancement post contrast administration (arrow).
NON-CANCEROUS ENTITIES
- Post biopsy hemorrhage
- Benign prostatic hyperplasia (BPH) nodule
- Acute and Chronic prostatitis
- Post inflammatory scars/fibrosis
- Atrophy
- Periprostatic lymph nodes
- Granulomatous prostatitis (GP)
Post biopsy Hemorrhage
- The prostate gland normally produces citrate which functions as an anticoagulant,
which makes hemorrhage in the prostate last longer after a biopsy.
- Hemorrhage usually causes signal intensity alterations in the gland making difficult the images interpretation.
- MRI Findings: Low signal on T2WI.
Heterogeneous appearance (Fig. 13).
- These findings can masquerade as a tumor.
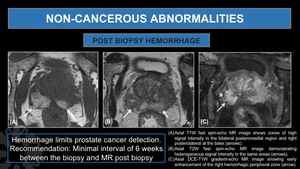
Fig. 13: Post Biopsy Hemorrhage
(A). Axial T1W fast spin-echo MR image shows zones of high signal intensity in the bilateral posteromedial region and right posterolateral at the base (arrows).
(B). Axial T2W fast spin-echo MR image demonstrating heterogeneous signal intensity in the same areas (arrows).
(C). Axial DCE-T1W gradient-echo MR image showing early enhancement of the right hemorrhagic peripheral zone (arrow).
Benign Prostatic Hyperplasia (BPH)
- One of the most common diseases of mankind.
Its prevalence increases with age: no reported in men younger than 30.
- Inflammation,
local or systemic,
can be an etiologic factor in the development of BPH.
- Obesity markedly increases the risk of developing BPH.
- The histologic subtypes of BPH include:
- Fibromuscular proliferation of stroma (Fig. 15)
- Glandular proliferation (Fig. 16)
- MRI Findings: Enlarged transition zone,
heterogeneous signal of the transition zone on T2WI and intact low signal pseudocapsule in the periphery.
BPH nodules could be hypo,
iso or hyperintense on T2Wi depending on the subtype (Fig. 14).
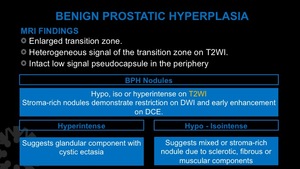
Fig. 14: Benign Prostatic Hyperplasia. MR Findings.
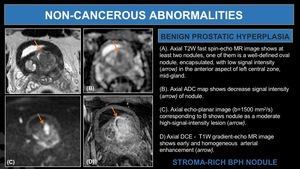
Fig. 15: Stroma-Rich BPH nodule.
(A). Axial T2W fast spin-echo MR image shows at least two nodules, one of them is a well-defined oval nodule, encapsulated, with low signal intensity (arrow) in the anterior aspect of left central zone, mid-gland.
(B). Axial ADC map shows decrease signal intensity (arrow) of nodule.
(C). Axial echo-planar image (b=1500 mm2/s) corresponding to B shows nodule as a moderate high-signal-intensity lesion (arrow).
D) Axial DCE - T1W gradient-echo MR image shows early and homogeneous arterial enhancement (arrow).
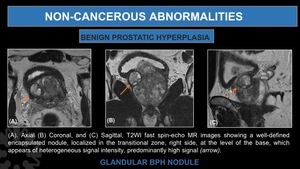
Fig. 16: Glandular BPH Nodule.
(A). Axial (B) Coronal, and (C) Sagittal, T2WI fast spin-echo MR images showing a well-defined encapsulated nodule, localized in the transitional zone, right side, at the level of the base, which appears of heterogeneous signal intensity, predominantly high signal (arrow).
Post inflammatory scars/fibrosis,
Acute and Chronic Prostatitis.
(Fig. 17,
Fig. 18)
- Most frequent benign pathologies as false positive in the PZ.
- In the absence of inflammatory symptoms
- Signal abnormalities in T2WI,
DWI,
and DCE.
- Up to 58% correspond to inflammatory changes.
Despite the superposition of inflammatory and tumor characteristics,
MP-MRI has a greater capacity to differentiate prostatitis from high-grade tumors.
- Prostatitis may have a lobar distribution or affect the peripheral zone diffusely.
- Scars tend to be triangular in shape.
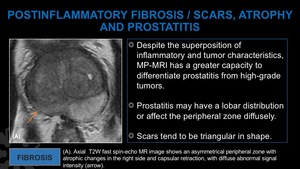
Fig. 17: Fibrosis.
(A). Axial T2W fast spin-echo MR image shows an asymmetrical peripheral zone with atrophic changes in the rigth side and capsular retraction, with diffuse abnormal signal intensity.
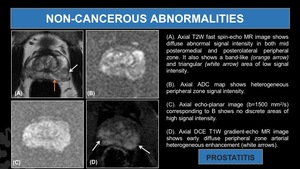
Fig. 18: Prostatitis.
(A). Axial T2W fast spin-echo MR image shows diffuse abnormal signal intensity in both mid posteromedial and posterolateral peripheral zone. It also shows a band-like (orange arrow) and triangular (white arrow) area of low signal intensity.
(B). Axial ADC map shows heterogeneous peripheral zone signal intensity.
(C). Axial echo-planar image (b=1500 mm2/s) corresponding to B shows no discrete areas of high signal intensity.
(D). Axial DCE T1W gradient-echo MR image shows early diffuse peripheral zone arterial heterogeneous enhancement (white arrows).
Atrophy
- Focal atrophy,
may mimic prostate malignancy at MRI due to its glandular crowding and complex glandular architecture
- Histologic subtypes include simple,
sclerotic with cyst formation,
and post-atrophic hyperplastic.
- MRI Findings: More frequent in the peripheral zone and appears as a focal or geographic area of low signal intensity on T2WI.
The degree of diffusion restriction and contrast enhancement is usually less than with prostate cancer ( Fig. 19 ).
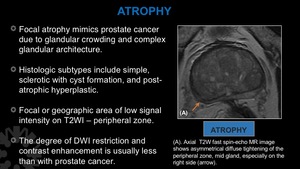
Fig. 19: Atrophy.
(A). Axial T2W fast spin-echo MR image shows asymmetrical diffuse tightening of the peripheral zone, mid gland, especially on the right side (arrow).
GRANULOMATOUS PROSTATITIS
( Fig. 21,
Fig. 22,
Fig. 23,
Fig. 24)
- GP is a benign inflammatory process rarely encountered in clinical practice.
- GP has a reported incidence of 0,36% in a study conducted by Oppenheimer et al.
in 25000 men who underwent needle biopsy of the prostate and within the inflammatory lesions of the prostate has a reported incidence of 3,3% affecting men in their sixth to eighth decades.
In the basis of histopathology findings and probable etiology GP is classified into non-specific (idiopathic),
specific (infectious),
iatrogenic (postsurgery),
malacoplakia and rarely with systemic causes (allergy and granulomatous diseases) being Non-specific granulomatous prostatitis the most common reported type.
- Infectious GP has been related with the use of intravesical Bacillus Calmette- Guerin (BCG) therapy,
an important adjunct in the therapy of bladder cancer.
It is presented as a complication of the treatment with a reported incidence between 1,3-40%(4,5).
- GP can be mistaken for prostatic Cancer,
both clinically and radiographically.
Patients with GP have shown elevated level of Serum PSA most affected by acute inflammation.
- In the other hand,
in the era of MP-MRI for detection and management of prostate cancer,
GP has also presented as a pathologic false-positive lesion on MP-MRI with moderate or high suspicion for prostatic malignancy.
- MP-MRI has demonstrated its ability to detect clinically significant cancer.
However,
there are benign conditions associated with false positives in MP-MRI categorized as suspicious with scores of 4 and 5 following the Prostate Imaging – Reporting and Data System Version 2 (PIRADS) guidelines.
Among these,
non-necrotic GP is described as a low signal discrete areas on T2WI and apparent diffusion coefficient (ADC) maps mimicking prostate cancer.
- Following contrast administration non-necrotic GP could present moderate or marked enhancement due to its highly cellular component.
Necrotic GP demonstrates an area of high signal intensity on T2WI with marked diffusion restriction without enhancement after contrast administration correspondent with central necrosis.
- Due to its inflammatory behavior,
GP can be associated with infiltration of the prostatic capsule,
simulating tumoral extraprostatic extension.
- In patients with histopathologic evidence of GP and concomitant prostate cancer,
it is difficult to distinguish if the MR findings correspond to the granulomatous disease or the cancer due to its similar appearance in MR imaging.
- There is an increasing need of identify the characteristics of GP in MP-MRI in order to improve its detection and obtain an accurate differentiation from PCa.
- MR Findings resume (Fig. 20).
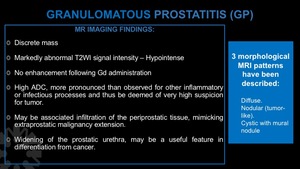
Fig. 20: Granulomatous Prostatitis MR Imaging Findings.

Fig. 21: Granulomatous Prostatitis.
(A) T2WI , (B) Dynamic contrast enhanced T1WI, (C) Diffusion weighted Images (DWI), and (D) Apparent Diffusion Coefficient (ADC) of the prostate, showing a focal area of mildly decreased T2 signal intensity, decreased ADC signal, and abnormal enhancement in the midgland - right transitional zone (highlighted in blue).
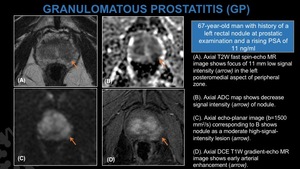
Fig. 22: Granulomatous Prostatitis.
(A). Axial T2W fast spin-echo MR image shows focus of 11 mm low signal intensity (arrow) in the left posteromedial aspect of peripheral zone.
(B). Axial ADC map shows decrease signal intensity (arrow) of nodule.
(C). Axial echo-planar image (b=1500 mm2/s) corresponding to B shows nodule as a moderate high-signal-intensity lesion (arrow).
(D). Axial DCE T1W gradient-echo MR image shows early arterial enhancement (arrow).
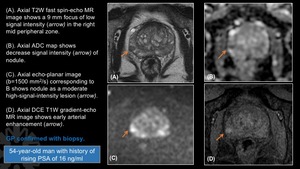
Fig. 23: Granulomatous Prostatitis.
(A). Axial T2W fast spin-echo MR image shows a 9 mm focus of low signal intensity (arrow) in the right mid peripheral zone.
(B). Axial ADC map shows decrease signal intensity (arrow) of nodule.
(C). Axial echo-planar image (b=1500 mm2/s) corresponding to B shows nodule as a moderate high-signal-intensity lesion (arrow).
(D). Axial DCE T1W gradient-echo MR image shows early arterial enhancement (arrow).
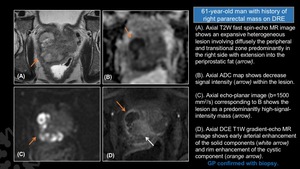
Fig. 24: Granulomatous Prostatitis.
(A). Axial T2W fast spin-echo MR image shows an expansive heterogeneous lesion involving diffusely the peripheral and transitional zone predominantly in the right side with extension into the periprostatic fat (arrow).
(B). Axial ADC map shows decrease signal intensity (arrow) within the lesion.
(C). Axial echo-planar image (b=1500 mm2/s) corresponding to B shows the lesion as a predominanltly high-signal-intensity mass (arrow).
(D). Axial DCE T1W gradient-echo MR image shows early arterial enhancement of the solid components (white arrow) and rim enhancement of the cystic component (orange arrow).
TECHNICAL CHALLENGES RELATED TO DWI
- Anatomic Distortion of High-b-Value DWI
- Lack of Suppression of Benign Prostate Tissue on Standard High-b-Value DWI
- Suboptimal Windowing of the ADC Map
Anatomic Distortion of High-b-Value DWI
- DWI usually uses a rapid switching of strong magnetic gradients,
which induces eddy currents and superimposed magnetic fields.
These eddy currents cause anatomical distortions when using a high b value.
- The distortion can be a change in the ones describe below,
compared to T2WI:
- Size
- Shape
- Position.
- This is a technical challenge because it can,
either hide or make look like,
a prostate cancer.
Lack of Suppression of Benign Prostate Tissue on Standard High-b-Value DWI
- The purpose of the high-b-value DWI is to create a visual contrast between what really is a tumor and the normal parenchyma of an organ.
In the prostate the value of b must be even greater than that used in other organs (500-1000 s/mm2),
because even at high-b-values,
the normal parenchyma of the gland continues to show signal.
- When MR exams are performed with the standard b-value for other organs,
it can cause errors in the interpretation,
leading whether to a false negative or a false positive.
Suboptimal Windowing of the ADC Map
- It is essential that the radiologist set the window and level of the image adequately in order to obtain the best quality and maximal visibility of the lesion.
- If the level is too high,
the low signal of the lesion could be under or over estimated.

. Axial and Sagittal T2W fast spin-echo MR images showing enlargement and thickening of the anterior fibromuscular stroma with low signal intensity (arrows).
(C). Axial ADC map shows mildly decrease signal intensity of the AFS (arrow).
(D). Axial DCE T1W gradient-echo MR image shows mild enhancement post contrast administration (arrow).")
. Axial T1W fast spin-echo MR image shows zones of high signal intensity in the bilateral posteromedial region and right posterolateral at the base (arrows).
(B). Axial T2W fast spin-echo MR image demonstrating heterogeneous signal intensity in the same areas (arrows).
(C). Axial DCE-T1W gradient-echo MR image showing early enhancement of the right hemorrhagic peripheral zone (arrow).")
. Axial T2W fast spin-echo MR image shows at least two nodules, one of them is a well-defined oval nodule, encapsulated, with low signal intensity (arrow) in the anterior aspect of left central zone, mid-gland.
(B). Axial ADC map shows decrease signal intensity (arrow) of nodule.
(C). Axial echo-planar image (b=1500 mm2/s) corresponding to B shows nodule as a moderate high-signal-intensity lesion (arrow).
D) Axial DCE - T1W gradient-echo MR image shows early and homogeneous arterial enhancement (arrow).")

. Axial (B) Coronal, and (C) Sagittal, T2WI fast spin-echo MR images showing a well-defined encapsulated nodule, localized in the transitional zone, right side, at the level of the base, which appears of heterogeneous signal intensity, predominantly high signal (arrow).")
. Axial T2W fast spin-echo MR image shows an asymmetrical peripheral zone with atrophic changes in the rigth side and capsular retraction, with diffuse abnormal signal intensity.")
. Axial T2W fast spin-echo MR image shows diffuse abnormal signal intensity in both mid posteromedial and posterolateral peripheral zone. It also shows a band-like (orange arrow) and triangular (white arrow) area of low signal intensity.
(B). Axial ADC map shows heterogeneous peripheral zone signal intensity.
(C). Axial echo-planar image (b=1500 mm2/s) corresponding to B shows no discrete areas of high signal intensity.
(D). Axial DCE T1W gradient-echo MR image shows early diffuse peripheral zone arterial heterogeneous enhancement (white arrows).")
. Axial T2W fast spin-echo MR image shows asymmetrical diffuse tightening of the peripheral zone, mid gland, especially on the right side (arrow).")

 T2WI , (B) Dynamic contrast enhanced T1WI, (C) Diffusion weighted Images (DWI), and (D) Apparent Diffusion Coefficient (ADC) of the prostate, showing a focal area of mildly decreased T2 signal intensity, decreased ADC signal, and abnormal enhancement in the midgland - right transitional zone (highlighted in blue).")
. Axial T2W fast spin-echo MR image shows focus of 11 mm low signal intensity (arrow) in the left posteromedial aspect of peripheral zone.
(B). Axial ADC map shows decrease signal intensity (arrow) of nodule.
(C). Axial echo-planar image (b=1500 mm2/s) corresponding to B shows nodule as a moderate high-signal-intensity lesion (arrow).
(D). Axial DCE T1W gradient-echo MR image shows early arterial enhancement (arrow).")
. Axial T2W fast spin-echo MR image shows a 9 mm focus of low signal intensity (arrow) in the right mid peripheral zone.
(B). Axial ADC map shows decrease signal intensity (arrow) of nodule.
(C). Axial echo-planar image (b=1500 mm2/s) corresponding to B shows nodule as a moderate high-signal-intensity lesion (arrow).
(D). Axial DCE T1W gradient-echo MR image shows early arterial enhancement (arrow).")
. Axial T2W fast spin-echo MR image shows an expansive heterogeneous lesion involving diffusely the peripheral and transitional zone predominantly in the right side with extension into the periprostatic fat (arrow).
(B). Axial ADC map shows decrease signal intensity (arrow) within the lesion.
(C). Axial echo-planar image (b=1500 mm2/s) corresponding to B shows the lesion as a predominanltly high-signal-intensity mass (arrow).
(D). Axial DCE T1W gradient-echo MR image shows early arterial enhancement of the solid components (white arrow) and rim enhancement of the cystic component (orange arrow).")