We retrospectively reviewed the CT and MRI examinations of 20 patients with spinal lymphoma,
18 NHL cases (4 primary/14 metastatic) and 2 patients with primary osseous HD,
performed within a 2-year-period.
The majority of patients were middle-aged,
with a slight male predilection.
NHL exhibited a lytic-destructive and multifocal/diffuse pattern in 15/18 patients,
half of which presented with accompanying soft-tissue mass [Fig 7]. A solitary lytic-metastatic lesion was seen in one case [Fig.8],
whereas multiple mixed sclerotic-lytic lesions were found in two patients [Fig.9, Fig.10].
There were no significant differences in imaging between primary and secondary spinal NHL.
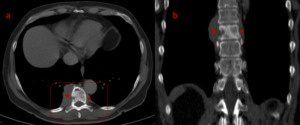
Fig. 7: Secondary spinal NHL: Axial CT image (a) demonstrates lymphomatous infiltration of the T9 vertebral body (outline), presenting as small lytic foci with associated focal cortical disruption, and accompanying extra-osseous soft-tissue mass surrounding the vertebra (asterisks), extending from the level of T8 to the level of T10 vertebra as shown on the coronal image (b), possibly infiltrating the right T9-T10 intervertebral foramen.

Fig. 8: CT during follow-up process in a case of T-NHL, portrays a solitary, well-defined, lytic bone lesion within the L1 vertebral body (arrows in axial [a] and sagittal [b] images). There is no cortical disruption or associated soft-tissue mass. This was a rare case of solitary osseous metastasis of NHL.

Fig. 9: Primary spinal NHL: Axial CT image (a) depicts an extended mixed sclerotic-lytic lesion of the sacrum (outline), with soft-tissue component projecting into the right S1-S2 intervertebral foramen causing enlargement and possible infiltration of the corresponding right exiting S1 root (arrow). There is also a left-sided soft-tissue lesion at the level of S2, projecting into the spinal canal, causing stenosis (asterisk), better demonstrated on the sagittal image (b).

Fig. 10: Initial work-up with CT (a) in a male patient presenting with persistent pelvic pain, demonstrates bone abnormalities in the right sacral ala and the adjacent part of the right ilium, with diffuse mixed sclerotic-lytic pattern (outline). Less profound findings can be seen on the left side of the sacrum. There is no bony expansion or sacroiliac joint deformity. Further imaging with MRI (b, c) depicts a diffusely low T1-signal in the sacrum, more prominent on the right side, also involving the ipsilateral ilium (b, asterisks), while on T2-WI (c) the corresponding areas appear inhomogeneous with multiple foci of increased signal. Differential diagnosis mainly includes metastases (especially from prostatic/testicular carcinoma), osseous lymphoma and Paget disease of the bone. Biopsy was conducted and histopathological results showed osseous DLBCL-NHL, although the blastic-sclerotic pattern is the less common type of bone lymphoma. 6-month follow-up CT image (d), after combined chemo-radiotherapy, portrays intense cortical sclerosis and more prominent sclerotic areas within the lesions (outline), possibly owing to radiation treatment. The affected regions are depicted as diffusely inhomogeneous on both T1-W(e) and T2-W (f) MR images, showing excessive hyperintense areas, more pronounced on the left part of the sacrum (arrows) compared to the initial study, indicating post-treatment fatty bone-marrow conversion.
Regarding the two cases with spinal HD,
one presented with prevertebral mass [Fig.11] and one with multifocal destructive osseous involvement [Fig12].
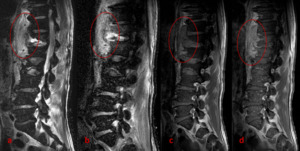
Fig. 11: Primary spinal lymphoma: MRI reveals a mass in the prevertebral space, extending from the level of T10 vertebra to the level of L2, in close contact with the anterior surface of T11-L1 vertebral bodies (outlines), appearing hyperintense on T2-W (a) and STIR (b) images and exhibiting lucid contrast enhancement on the post-contrast T1-WI (d) compared to the pre-contrast T1-WI (c). There is moderate edema at the anterior – inferior aspect of the T12 vertebral body better depicted on the T2-W (a) and STIR (b) images, with incipient bone erosion, but no contrast enhancement (d).
Observe the common imaging characteristics of the lesion with an inflammatory process, yet there was no evidence of spondylodiscitis.

Fig. 12: Primary multifocal spinal Hodgkin lymphoma: Sagittal STIR MR image (a) displays a diffusely homogeneous hyperintense C7 vertebral body (outline). There are also multiple lesions in the thoracic/thoracolumbar spine, as demonstrated on sagittal T1-W (b) and T2-W (c) images, with diffuse infiltration of the T10 and T11 vertebral bodies (b,asterisks) and presence of pathologic tissue extending in the adjacent posterior epidural space, effacing the corresponding subarachnoid space and causing moderate spinal cord compression (white arrows). There are also well-defined focal hypointense lesions within the T6 and L1 vertebral bodies (red arrows) and possible infiltration of the anterior-superior aspect of the T12 vertebral body (outlines).
Epidural/intradural infiltration was depicted in two NHL cases with available MRI [Fig.13].
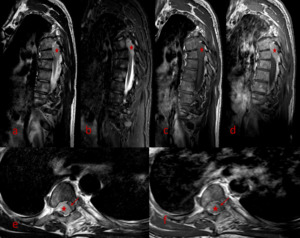
Fig. 13: Intradural spinal lymphoma: Sagittal T2-W (a), STIR (b), T1-W (c) and contrast-enhanced T1-W (d) MR images show a well-defined solid, homogeneously enhancing mass within the thecal sac at the upper thoracic spine (asterisks). Note the associated severe spinal cord compression, mostly at the T6 level, better depicted on axial T2-W (e) and contrast-enhanced T1-W (f) sequences (arrows).
Most of spinal lymphomas lacked specific appearance and were in some cases initially misdiagnosed as metastatic carcinoma,
multiple myeloma and rarely as inflammatory disorder [Fig.14].

Fig. 14: Primary spinal lymphoma: Sagittal STIR MR images at different levels (a, b, c) reveal multiple increased signal foci in the vertebral bone-marrow (arrows/outlines). High signal of bone-marrow in the anterior and posterior corner of a vertebra (outlines) mimics seronegative spondyloarthitis. However, in this case, biopsy revealed primary NHL.
