MRI imaging protocol
In general,
the main objective of the magnetic resonance protocol in the acute setting is to reduce the acquisition time without impairing the quality of the images.
This is made by reducing the number of sequences obtained and individualizing the breath-hold techniques according to the individual's clinical condition.
Illustrative cases from our department were collected and classified according to these pattern types.
Clinical and radiology presentations,
differential diagnosis,
and teaching points were also described.
FEMALE PELVIC EMERGENCIES
A.
Pelvic Inflammatory Disease
Review
Pelvic inflammatory disease (PID) is an infection of the woman's reproductive tract (endometrium,
fallopian tubes,
ovaries,
and peritoneum).
The clinical and imaging picture is variable,
depending on the stage and presentation of the disease.
The radiologist's role in emergencies is to identify complications that require immediate treatment.
The impact of PID involves both the acute life-threatening phase and the chronic phase which may result in infertility,
ectopic pregnancy,
and chronic pelvic pain.
Radiologic Findings
Endometritis: thickening and edema of the endometrium (best seen at T2-weighted images),
gas in endometrial cavity,
and intense mucosal enhancement on postcontrast T1-weighted images.
Pyosalpinx: the fallopian tube is characterized by distention by heterogeneous high T2 signal fluid that shows an important diffusion restriction,
and thick enhancement of the wall.
Tubo-ovarian abscess: complex pelvic mass with septations,
thick walls with enhancement,
fat stranding,
and edema.
Sometimes,
it can be difficult to differentiate from a malignant mass.
Case 1: A 21-years-old woman with 1-week history of abnormal vaginal discharge,
fever and low abdominal pain (Fig.
1).
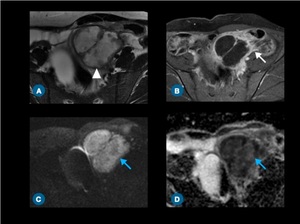
Fig. 1: (A) Axial T2-weighted and (B) postcontrast T1-weighted MR images demonstrate a complex cyst in the left adnexal region (white arrowhead) with strong enhancement of thick walls (white arrow). (C) Diffusion-weighted imaging and (D) ADC map show intense diffusion restriction (blue arrows).
References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo, São Paulo/BR.
Case 2: A 29-year-old woman presents to the emergency with fever and lower abdominal pain (Fig.
2).
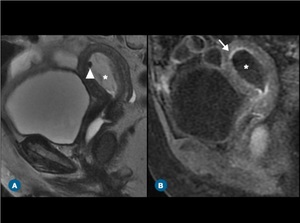
Fig. 2: (A) T2-weighted and (B) postconstrast T1-weighted MR images on sagittal plane show mild heterogenous distention of endometrial cavity (*) with gas (arrowhead) and thin enhancement of endometrium mucosa (arrow).
References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo, São Paulo/BR.
Case 3: A 30-year-old sexually active woman with fever and lower abdominal pain (Fig.
3).
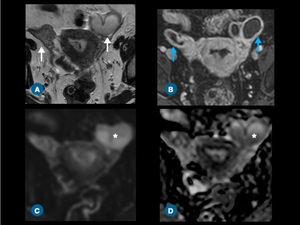
Fig. 3: (A) T2-weighted image and (B) postcontrast T1-weighted image demonstrate bilateral distention of fallopian tubes (white arrows) with strong wall enhancement (blue arrows). (C) Diffusion-weighted imaging and (D) ADC map show a slightly diffusion restriction (*).
References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo, São Paulo/BR.
Ovarian Emergency
B.
Ovarian Cyst Rupture
Review
Functional ovarian cysts are common in women of reproductive age,
most of then will not cause symptom and usually resolve in 4 - 8 weeks.
Due to high prevalence,
ruptured ovarian cysts are one of the most frequent causes of acute pelvic pain in premenopausal women.
This event is usually self-limiting,
however,
in some cases there might be significant hemoperitoneum,
requiring a surgical approach.
Furthermore,
other ovarian lesions can rupture,
being the most common the mature cystic teratoma.
Radiologic Findings
The ovarian lesion ruptured changes the appearance with a distorted shape and irregular wall thickening.
Free fluid due to the leaking of lesion content and peritonitis also can be seen.
Case 4: A 33-years old woman with acute epigastric pain and syncope.
(Fig.
4).
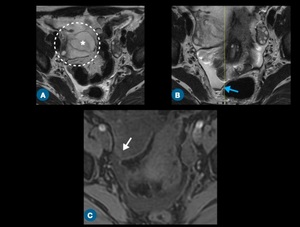
Fig. 4: (A,B) Axial T2-weighted images show an irregular cyst (*) within the enlarged right ovary (dashed circle), surrounded by slightly blood content characterized on (C) T1-weighted image (white arrow). Free fluid with blood content (blue arrow) is also seen.
References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo, São Paulo/BR.
C.
Ovarian Torsion
Review
Ovarian torsion consists of a partial or complete twist of the pedicle that causes vascular impairment.
It usually happens among women of reproductive age and is frequently related to benign ovarian tumors like mature teratoma,
and follicular or corpus luteal cysts.
Massive ovarian edema (MOE) secondary to ovarian torsion occurs by impairment of venous and lymphatic drainage.
This pathology occurs mainly in young women and is usually confused with a tumor.
Radiologic Findings
The most common MR imaging features are the enlargement and edema of the ovary that is an indirect finding.
The twisted pedicle and fallopian tube thickening are direct findings of ovarian torsion.
Sometimes,
the twisted pedicle appears like a mass-like lesion in the adnexal region.
The vascular impairment first causes an interruption of venous and lymphatic outflow,
resulting in ovarian edema and thickening of the fallopian tube.
In the second moment,
the arterial blood flow is interrupted and causes ischemia and hemorrhagic infarction (minimal or absent enhancement).
The main features of MOE are multiple peripheral follicles in an enlarged ovary characterized by intense stromal edema seen on T2-weighted images.
Case 1: A 24-year-old woman presents to the emergency with severe pelvic pain,
nausea,
and anorexia (Fig.
5).
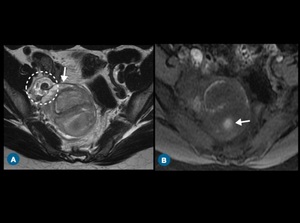
Fig. 5: Axial MRI images demonstrate the enlargement of the right ovary with (A) high signal on T2-weighted image (edema) and blood content on T1-weighted-image (hemorrhagic infarction). A twisted vascular pedicle is also seen (dashed circle).
References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo, São Paulo/BR.
Case 2: A 22-years-old woman with self-limited abdominal pain associated with a palpable mobile adnexal mass on physical examination (Fig.
6).
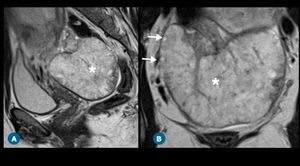
Fig. 6: (A) Sagittal and (B) coronal T2-weighted MR images show some small follicles (arrow) at the periphery of the enlarged ovary (*). Note the intense stromal edema.
References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo, São Paulo/BR.
D.
Fibroid Degeneration and Torsion
Review
Uterine fibroid are benign smooth muscle cell tumors,
and one of the most common pelvic neoplasm.
Most often they are asymptomatic but may promote some disorders,
such as uterine bleeding,
iron deficiency,
compression,
degeneration,
and torsion.
Generally,
leiomyomas progress to hyaline degeneration (more than 60% of cases).
Red degeneration is caused by venous thrombosis within the periphery of the lesion and may promote acute abdominal pain.
This disease usually occurs during pregnancy and its associated with oral contraception.
Subserosal uterine leiomyoma torsion is rare and causes acute pelvic pain.
Main differential diagnoses are uterine torsion and ovarian torsion.
Radiologic findings
Leiomyoma red degeneration is typically a non-vascularized,
well-defined uterine mass surrounded by normal enhancement of myometrium.
It may appear as peripheral or diffuse hyperintensity on T1-weighted images.
The entire lesion shows a minimal or absent enhancement.
The subserosal leiomyoma torsion demonstrates imaging features similar to the red degeneration.
In addition,
it may show a twisted pedicle but is difficult to identify because the twisted pedicle is thin.
In these cases,
is crucial the visualization of normal ovaries to avoid misinterpretation (eg,
endometrioma,
ovarian tumors).
Case 1: A 40-year-old premenopausal woman presents to the emergency with nausea,
vomiting and low abdominal pain (Fig.
7).
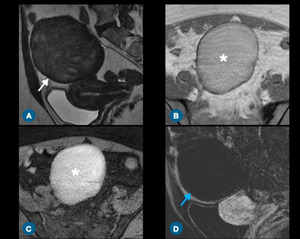
Fig. 7: (A) Sagittal T2-weighted MR imaging shows a large leiomyoma with low signal (white arrow). Axial T1-weighted images on (B) in-phase sequence and (C) fat suppressed sequence demonstrate hypersignal with absent contrast enhancement after gadolinium administration (D) on postcontrast T1-weighted image in subtraction technique (blue arrow).
References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo, São Paulo/BR.
Case 2: A 33-year-old woman with sudden onset pain in the right flank (Fig.
8).
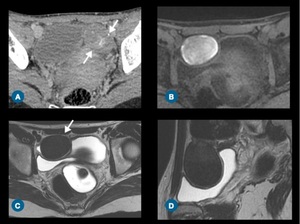
Fig. 8: (A) Axial contrast enhanced CT scan shows a mass in the left adnexal region with thin calcifications (arrows). MR images two days after CT demonstrate a well-defined lesion in the right adnexal region with (B) high signal on T1-weighted image and (C,D) low signal on T2-weighted image. The findings suggest torsion of a pedunculated uterine leiomyoma with red degeneration.
References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo, São Paulo/BR.
Pregnancy-related Disorders
E.
Ectopic Pregnancy
Review
Ectopic pregnancy is a high morbidity and mortality disorder,
being one of the main causes of maternal death in the first trimester.
It occurs when there is implantation of the blastocyst outside the uterus endometrium.
Most frequent,
the ectopic pregnancy is in the ampullary region of the fallopian tube,
however,
there is the possibility of implantation in other sites,
such as ovaries,
abdominal cavity,
and uterine scar of cesarean.
Radiologic Findings
MR findings may be non-specific,
but clinical history and laboratory exams help the interpretation.
Tubal pregnancy appears as an adnexal cystic lesion that is separate from the normal ovary.
Blood component can be observed if the ectopic gestation ruptures,
most commonly as bloody ascites and,
hematosalpinx.
Case: A 27-year-old woman with lower abdominal pain,
vaginal bleeding and menstrual delay (hCG level of 440.0 mIU/mL) (Fig.
9).
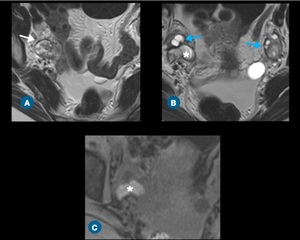
Fig. 9: (A,B) Axial T2-weighted and (C) precontrast T1-weighted MR images show a sac-like mass in the right adnexal region (white arrow) and a normal ovaries (blue arrows). Hematosalpingx (*) is also seen (B,C).
References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo, São Paulo/BR.
F.
Retained Products of Conception and Arteriovenous Fistula
Review
Retained product of conception (RPOC) and arteriovenous (AV) fistula are a common cause of delayed postpartum hemorrhage (PPH) and both are differential diagnoses.
RPOC is characterized by persistence of placental or trophoblastic tissues after pregnancy delivery or abortion.
The AV fistula is a rare condition,
but typically described as a hypervascular lesion in a patient with a negative hCG.
These diseases cause pelvic pain and uterine bleeding.
Radiologic findings:
The RPOC appearance is a mass with various degrees of vascularity in the endometrium to the myometrium interface,
characterized by polypoid lesion with a heterogeneous signal at T1 and T2-weighted images at MR.
In consequence of marked vascularity,
some cases of RPOC are misinterpreted as AV fistula.
To avoid misdiagnosis,
a typical sign is frequently seen in the AV fistula that is an increasingly enhanced structure in the myometrium with extension to endometrium on arterial phase,
interpreted as tubular flow voids on non-contrast T1 and T2-weighted images.
Case 1: A 30-years-old woman with vaginal bleeding and dizziness.
She had a history of vaginal delivery 4 weeks earlier (Fig.
10).

Fig. 10: At MR, a polypoid, heterogeneous lesion into the endometrial cavity on (A) sagittal T2-weighted image (white arrow), associated with wispy contrast enhancement on (B) sagittal T1-weighted image (blue arrow). Note a slight ill definition of endometrial-myometrial interface.
References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo, São Paulo/BR.
Case 2: A young female with curettage history a month ago due to abortion.
Now with sudden excessive vaginal bleeding and syncope (Fig.
11).

Fig. 11: (A) Sagittal T2-weighted and (B) axial unenhanced T1-weighted MR images show uterine cavity distend by heterogeneous, hemorrhagic fluid (white arrows). An intense enhancement of endometrial-myometrial interface (arrowheads) is seen on (C) postcontrast T1-weighted image (arterial) associated with early opacification of gonadal veins (blue arrows).
References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo, São Paulo/BR.
G.
Acute Appendicitis in Pregnancy
Review
Appendicitis is the most common non-obstetric cause of emergency during pregnancy,
especially at the second trimester.
Sometimes this inflammatory disease may become a challenging diagnosis due to nonspecific leukocytosis,
pain,
and displacement of the appendix as a result of gravid uterus.
Radiologic findings
MR features of appendicitis are a diameter greater than 7 mm,
wall thickening greater than 2 mm,
internal content with high signal on T2-weighted images due to fluid or edema,
periappendiceal fluid,
and fat stranding.
Case: A 28-years-old woman G3P2 at 12 weeks gestational age presented at the emergency room with a 2-day history of diffuse abdominal pain (Fig.
12).
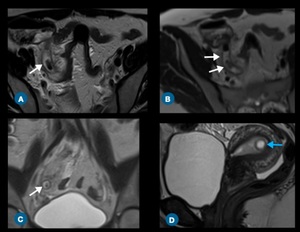
Fig. 12: (A,B) Axial and (C) coronal T2-weighted MR images show an inflamed and enlarged appendix (white arrows). (D) Sagittal T2-weighted image demonstrates the gestational sac (blue arrow).
References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo, São Paulo/BR.
MALE PELVIC EMERGENCIES
Penile and Prostatic Disorders
H.
Penile Prosthesis Fracture
Review
The use of penile prosthesis has increased in recent years,
currently being the third line of therapy for erectile dysfunction and as a complement in penile reconstructions in transsexual patients.
Late complications prosthesis-related include infection,
displacement,
and fracture of the prosthesis.
Radiologic findings
Prosthesis discontinuity is better evaluated on T1-weighted images,
surrounded by hematoma/edema,
and with cylinders malpositioning.
Case: A 54-year-old man with semirigid penile prosthesis implantation presented to the emergency after noting penile deformity and pain during sexual intercourse (Fig.
13).
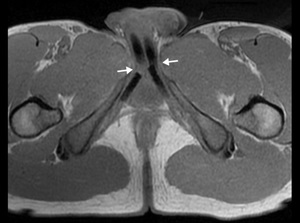
Fig. 13: Axial T1-weighted MR image demonstrates a fractured of penile prosthesis implantation (arrows).
References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo, São Paulo/BR.
I) Priapism
Review
Priapism is defined as a prolonged (often painful) erection,
longer than 4 hours and unrelated to sex activity.
There are many causes involved in this condition,
such as phosphodiesterase inhibitors,
sickle cell anemia,
trauma,
and idiopathic causes.
The main role of the radiologist is to differentiate the high flow priapism from low flow priapism.
Low flow priapism is the most common form and requires quick treatment because may cause compartment syndrome.
Radiologic findings
In low-flow priapism,
the degree of corporal infarction is seen on T1 and T2-weighted images.
The perfusion of the corpora can be slow,
so delayed postcontrast sequences are necessary to assess tissue viability.
In high flow type,
the fistula can be characterized on dynamic postcontrast sequences.
The T2-weighted images usually demonstrate a heterogeneous focus of flow void,
and postcontrast phase demonstrates an asymmetric,
early enhancement in the corpus of the same side.
Case: A 32-year-old male who presented to the emergency after a straddle injury (Fig.
14).
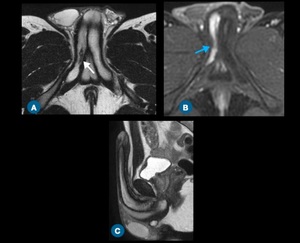
Fig. 14: (A) Axial T2-weighted MR image shows a focal lesion (white arrow) in the right corpora cavernosa. (B) Postcontrast T1-weighted image on arterial phase demonstrates earlier, asymmetric enhancement in the right corpus cavernosum.
References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo, São Paulo/BR.
J) Prostatic Abscess
Review
Prostatic abscess is a rare and difficult diagnosis because the symptoms are nonspecific.
Often the clinical presentation is confused with other diseases of the lower urinary tract.
The incidence has decreased because of early antibiotic therapy.
The most common organisms involved are E coli and Staphylococcus.
This disease is frequently diagnosed in elderly patients with preexisting chronic obstructive troubles or urinary episodic inflammation.
Radiologic Findings
MR features include a liquefied lesion characterized by a high heterogeneous signal on T2-weighted images,
a variable degree of diffusion restriction,
and ringlike enhancement.
Case: A 50-year-old man with untreated diabetes and urinary symptoms (Fig.
15).
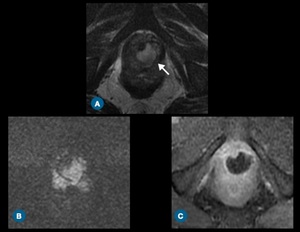
Fig. 15: A cystic lesion in the prostatic apex demonstrating hyperintensity on (A) T2-weighted image, associated with (B) diffusion restriction, and (C) ringlike enhancement on T1-weighted image.
References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo, São Paulo/BR.

 Axial T2-weighted and (B) postcontrast T1-weighted MR images demonstrate a complex cyst in the left adnexal region (white arrowhead) with strong enhancement of thick walls (white arrow). (C) Diffusion-weighted imaging and (D) ADC map show intense diffusion restriction (blue arrows). References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo, São Paulo/BR.")
 T2-weighted and (B) postconstrast T1-weighted MR images on sagittal plane show mild heterogenous distention of endometrial cavity (*) with gas (arrowhead) and thin enhancement of endometrium mucosa (arrow). References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo, São Paulo/BR.")
 T2-weighted image and (B) postcontrast T1-weighted image demonstrate bilateral distention of fallopian tubes (white arrows) with strong wall enhancement (blue arrows). (C) Diffusion-weighted imaging and (D) ADC map show a slightly diffusion restriction (*). References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo, São Paulo/BR.")
 Axial T2-weighted images show an irregular cyst (*) within the enlarged right ovary (dashed circle), surrounded by slightly blood content characterized on (C) T1-weighted image (white arrow). Free fluid with blood content (blue arrow) is also seen. References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo, São Paulo/BR.")
 high signal on T2-weighted image (edema) and blood content on T1-weighted-image (hemorrhagic infarction). A twisted vascular pedicle is also seen (dashed circle).
References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo, São Paulo/BR.")
 Sagittal and (B) coronal T2-weighted MR images show some small follicles (arrow) at the periphery of the enlarged ovary (*). Note the intense stromal edema. References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo, São Paulo/BR.")
 Sagittal T2-weighted MR imaging shows a large leiomyoma with low signal (white arrow). Axial T1-weighted images on (B) in-phase sequence and (C) fat suppressed sequence demonstrate hypersignal with absent contrast enhancement after gadolinium administration (D) on postcontrast T1-weighted image in subtraction technique (blue arrow).
References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo, São Paulo/BR.")
 Axial contrast enhanced CT scan shows a mass in the left adnexal region with thin calcifications (arrows). MR images two days after CT demonstrate a well-defined lesion in the right adnexal region with (B) high signal on T1-weighted image and (C,D) low signal on T2-weighted image. The findings suggest torsion of a pedunculated uterine leiomyoma with red degeneration. References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo, São Paulo/BR.")
 Axial T2-weighted and (C) precontrast T1-weighted MR images show a sac-like mass in the right adnexal region (white arrow) and a normal ovaries (blue arrows). Hematosalpingx (*) is also seen (B,C). References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo, São Paulo/BR.")
 sagittal T2-weighted image (white arrow), associated with wispy contrast enhancement on (B) sagittal T1-weighted image (blue arrow). Note a slight ill definition of endometrial-myometrial interface. References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo, São Paulo/BR.")
 Sagittal T2-weighted and (B) axial unenhanced T1-weighted MR images show uterine cavity distend by heterogeneous, hemorrhagic fluid (white arrows). An intense enhancement of endometrial-myometrial interface (arrowheads) is seen on (C) postcontrast T1-weighted image (arterial) associated with early opacification of gonadal veins (blue arrows). References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo, São Paulo/BR.")
 Axial and (C) coronal T2-weighted MR images show an inflamed and enlarged appendix (white arrows). (D) Sagittal T2-weighted image demonstrates the gestational sac (blue arrow). References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo, São Paulo/BR.")
. References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo, São Paulo/BR.")
 Axial T2-weighted MR image shows a focal lesion (white arrow) in the right corpora cavernosa. (B) Postcontrast T1-weighted image on arterial phase demonstrates earlier, asymmetric enhancement in the right corpus cavernosum. References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo, São Paulo/BR.")
 T2-weighted image, associated with (B) diffusion restriction, and (C) ringlike enhancement on T1-weighted image. References: INRAD, Hospital das Clínicas da Faculdade de Medicina de São Paulo, São Paulo/BR.")