A retrospective study of 15 years including 180 patients,
aged 1- 80 years who have undergone a thoracic CT exam,
performed without and with contrast injection,
followed by MPR reconstructions in coronal and sagittal plane,
for suspicion of anterior mediastinal masses or in the context of myasthenia gravis/ myasteniform syndrome.
In the current study,
60 patients had normal thymic features,
whilst 120 patients presented with anterior mediastinal masses.
The dominant pathologies were lymphoma and thymoma.
NORMAL THYMUS
Normal CT features of the thymus gland
The thymus is located in the anterior mediastinum,
and extends approximatively 1.7 cm superiorly to the innominate vein,
and inferiorly to the pulmonary arteries in adults.
In infants,
it may reach the diaphragm [7].
Its maximum anteroposterior diameter before the age of 20 years is 18 mm,
whilst after this age it is 13 mm [7].
Before puberty,
the shape is quadrilateral or triangular with convex lateral borders.
In adults,
the shape remains triangular or arrowhead,
but the margins become linear or concave.
The structure is homogenous,
with soft tissue attenuation in the pediatric population.
After puberty,
the density decreases,
and the structure becomes slightly heterogeneous.
Frequently,
after the age of 40 years,
complete fatty involution occurs.
Residual thymic tissue may also be present,
in the form of linear or oval-shaped tissue attenuating mass in the thymic loch [8]. Fig. 2
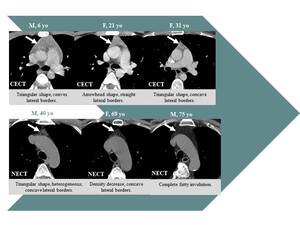
Fig. 2: Age related normal aspects of the thymus.
References: Department of Radiology and Medical Imagistics, Fundeni Clinical Institute/ Bucharest
THYMIC PATHOLOGY
Thymic hyperplasia
On CT,
rebound hyperplasia is a diffuse,
symmetric enlargement of the thymus,
without contour irregularities or focal masses.
The structure might be slightly heterogeneous through the presence of areas of intralesional fat [9].
Fig. 3
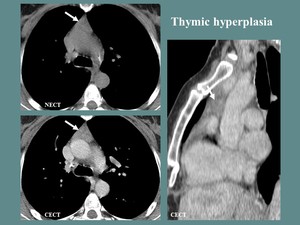
Fig. 3: F, 50 yo, history of chemotherapy for neuroendocrine pancreatic tumor. CT aspects: diffuse enlargement of the thymus, WITHOUTH contour irregularities or focal masses.
References: Department of Radiology and Medical Imagistics, Fundeni Clinical Institute/ Bucharest 2017
In lymphoid hyperplasia,
the thymus may have a normal appearance,
increased size,
or even a focal mass [7].
Thymic cysts
On CT,
the thymic cyst frequently presents as a fluid/ parafluid lesion [2],
but may also have higher densities (depending on the presence of blood products).
It is round or oval shaped,
with thin walls with or without calcified rims.
It shows no solid components or contrast enhancement.
Fig. 4
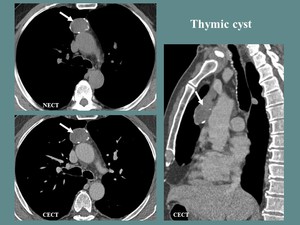
Fig. 4: M, 65 yo, myasthenia gravis. CT aspects: oval shaped parafluid mass, with thin walls and calcified rims. NO contrast enhancement.
References: Department of Radiology and Medical Imagistics, Fundeni Clinical Institute/ Bucharest 2015
Thymic epithelial tumors
Thymoma presents as a round,
oval or lobulated,
well outlined,
soft tissue mass,
frequently homogenous but may include calcifications,
cystic or necrotic areas [2]. Fig. 5
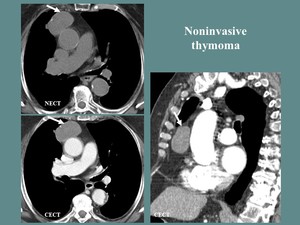
Fig. 5: M, 78 yo, myasthenia gravis. CT aspects: oval shaped, well outlined, soft tissue mass, nodular calcifications included.
References: Department of Radiology and Medical Imagistics, Fundeni Clinical Institute/ Bucharest 2014
Indicators of invasiveness in the context of thymoma are infiltration of the fat planes,
invasion of the great mediastinal vessels and pleural involvement (thickening,
nodularity or effusion) [3].
Fig. 6
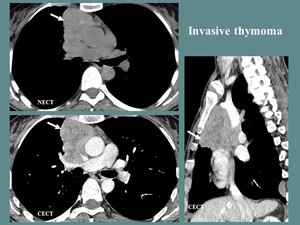
Fig. 6: F, 42 yo, myasthenia gravis. CT aspects: lobulated, well outlined, anterior mediastinum mass, with heterogeneous contrast enhancement (necrotic areas), undelimited and with compression of the ascending aorta and right pulmonary artery, surrounding the superior vena cava (more than 67% of the circumference).
References: Department of Radiology and Medical Imagistics, Fundeni Clinical Institute/ Bucharest 2017
Thymic carcinoma frequently presents as a large multilobulated soft tissue mass,
with heterogeneous enhancement,
local invasiveness (of the mediastinal fat,
great vessels,
pleura or lung),
associated lymphadenopathies and hematogenous dissemination [7].
Fig. 7
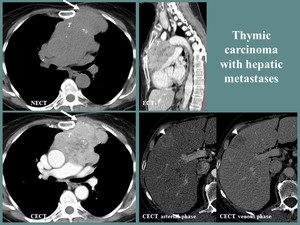
Fig. 7: F, 61 yo, dermatomyositis and anterior thoracic pain. CT aspects: large, lobulated thymic mass (T), heterogeneous, with central necrosis and nodular calcifications, invading the anterior thoracic wall (white arrow), with hypervascular hepatic metastases (arrowhead).
References: Department of Radiology and Medical Imagistics, Fundeni Clinical Institute/ Bucharest 2018
Germinal cell tumors
The CT aspects of germinal cell tumors are highly variable depending of the subtype of tumor. Thus,
a mature teratoma is intensely heterogeneous,
frequently associating cystic,
fat,
soft tissue and calcium densities,
seminomas are generally homogenous and nonseminomatous germ cell tumors are heterogeneous due to necrosis and hemorrhage [11]. Table 3, Fig. 8 ,
Fig. 9
| Mature teratoma |
Seminoma |
Nonseminomatous tumors |
|
Round/ lobulated mass.
Heterogeneous:
tissue,
cystic (fluid,
lipid,
mixt components),
calcar
elements (calcifications,
bone,
teeth).
Contrast enhancement
of the capsule and septa.
Extension towards
ONLY one side of the
median line.
|
Large,
lobulated, well
outlined.
Frequently
homogenous.
Extension towards
BOTH sides of the median line.
Local invasiveness.
Lymphogenous and hematogenous
metastatic disease.
|
Large,
lobulated,
well
outlined,
regular or
irregular borders.
Heterogeneous:diminished/ no central enhancement
(necrosis,
hemorrhage),
important peripheral
contrast enhancement.
Local invasiveness.
Lymphogenous and
hematogenous metastatic disease.
Pleural/pericardial
effusions.
|
Table 3. Main CT aspects in germinal cell tumors [11].
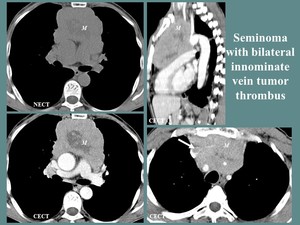
Fig. 8: M, 51 yo, anterior thoracic pain. CT aspects: lobulated, well outlined anterior mediastinal mass (M), with central necrosis, without visualization of the left innominate vein and tumor thrombosis at the confluence of the innominate veins (white arrow), including the brachiocephalic artery, left common carotid and subclavian artery, invading the anterior wall of the pulmonary trunk.
References: Department of Radiology and Medical Imagistics, Fundeni Clinical Institute/ Bucharest 2010

Fig. 9: M, 25 yo, thoracic pain, dry cough, fever, elevated α- fetoprotein. CT aspects: large, lobulated, well outlined anterior mediastinum mass (M), with extension towards the left side of the median line, highly heterogeneous, with central necrotic and hemorrhagic areas (white arrow) and peripheral contrast enhancement, nodular calcifications, hemothorax (arrowhead).
References: Department of Radiology and Medical Imagistics, Fundeni Clinical Institute/ Bucharest 2018
Thymic lymphoma and leukemia
Thymic involvement in lymphoma or leukemia presents as a soft tissue lobulated thymic mass,
frequently homogenous (may also include cystic or necrotic changes),
with mild contrast enhancement and local invasiveness,
surrounding the great vessels but commonly without invasion.
An important imagistic feature is the presence of associated lymphadenopathies.
Fig. 10 ,
Fig. 11 and Fig. 12
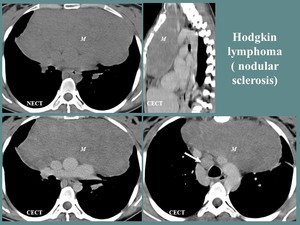
Fig. 10: F, 24 yo, anterior thoracic pain. CT aspects: large, homogeneous anterior mediastinum mass (M), in contact with the great mediastinal vessels, invading the fat planes, with important mass effect and posterior displacement of the mediastinal vessels, associated lymphadenopathies (white arrow).
References: Department of Radiology and Medical Imagistics, Fundeni Clinical Institute/ Bucharest 2011
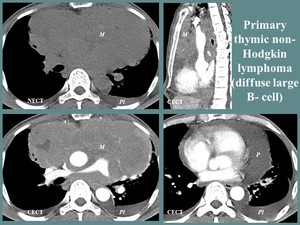
Fig. 11: M, 50 yo, dysphonia, dyspnea, cough, thoracic pain. CT aspects: large, lobulated, slightly heterogeneous (necrotic areas) mass (M), originating in the anterior mediastinum, with middle and posterior mediastinum extension, surrounding the great vessels but WITHOUTH invasion, associated bilateral pleurisy (Pl) and pericarditis (P).
References: Department of Radiology and Medical Imagistics, Fundeni Clinical Institute/ Bucharest 2018
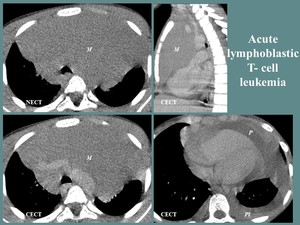
Fig. 12: M, 8 yo, weight loss (5 kg in 4 weeks), cervical lymphadenopathies. CT aspects: large, well outlined, homogeneous anterior mediastinum mass (M), invading the fat planes adjacent to the great vessels and pericardium, pleural (Pl) and pericardial effusion (P).
References: Department of Radiology and Medical Imagistics, Fundeni Clinical Institute/ Bucharest 2017
DIFFERENTIAL DIAGNOSIS
Differential diagnosis of the anterior mediastinum masses can be summarized using the mnemonic “4T”: thymoma,
teratoma,
thyroid tumors/ goiter,
and terrible lymphoma.
Other differential diagnoses
- Goiter can be diagnosed certainly by CT alone.
It appears as a lobulated anterior mediastinum mass,
frequently in continuity with the thyroid gland,
with high attenuation on non-contrast CT (70-85 UH) and prolonged contrast enhancement.
It is commonly inhomogeneous due to cystic changes and calcifications [9].
- Lymph node involvement secondary to extramediastinal malignancies [12].
- Ascending aorta aneurysms [14]. Fig. 13, Fig. 14 and Fig.
15
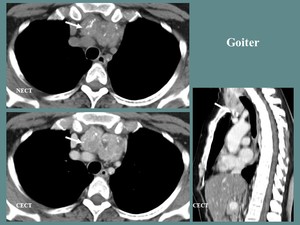
Fig. 13: F, 49 yo. CT aspects: lobulated, heterogeneous, high native attenuation, contrast enhancing anterior mediastinum mass, in continuity with the thyroid gland (white arrow).
References: Department of Radiology and Medical Imagistics, Fundeni Clinical Institute/ Bucharest 2013
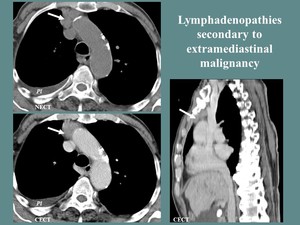
Fig. 14: M, 80 yo, diagnosed with hepatocarcinoma. CT: lymphadenopathies of the anterior mediastinum (white arrow), right pleural effusion (Pl).
References: Department of Radiology and Medical Imagistics, Fundeni Clinical Institute/ Bucharest 2012
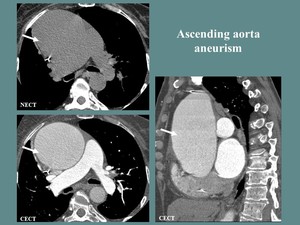
Fig. 15: F, 68 yo. EKG gating Angio-CT of the thoracic aorta: Important ascending aorta dilation, with no intraluminal defects (white arrow).
References: Department of Radiology and Medical Imagistics, Fundeni Clinical Institute/ Bucharest 2017
In particular cases,
secondary mediastinal involvement such as:
- lung malignancies with mediastinal extensions or
- anterior mediastinal plasmacytoma [13] should be taken into consideration.
Fig. 16 ,
Fig.
17
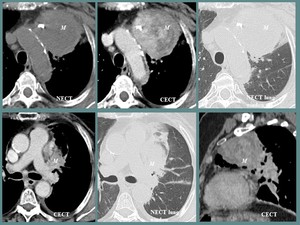
Fig. 16: Fig. 14. F, 63 yo, anterior thoracic pain, dyspnea. CT aspects: round, well outlined with slightly irregular contours, heterogeneous mass (M) involving the left pulmonary hilum and the anterior mediastinum, nodular calcifications. Histopathologic diagnosis: squamous cell pulmonary carcinoma.
References: Department of Radiology and Medical Imagistics, Fundeni Clinical Institute/ Bucharest 2012
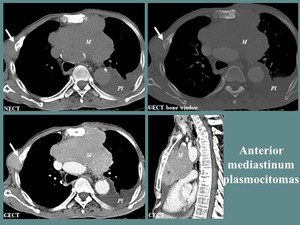
Fig. 17: M, 73 yo, diagnosed with multiple myeloma. CT aspects: large, lobulated, homogeneous anterior mediastinum mass (M), with extension to the middle mediastinum, left pleural effusion (Pl), associated bone lesions and right chest wall mass (white arrow).
References: Department of Radiology and Medical Imagistics, Fundeni Clinical Institute/ Bucharest 2012
STRUCTURED REPORT
The structured CT report in patients with myasthenia gravis,
miasteniform syndrome or suspicion of anterior mediastinal mass should include:
1.
Information regarding the anterior mediastinal mass :
- Location ;
- Size ;
- Contours : well outlined/ poorly outlined,
regular/ irregular contours ;
- Structure: homogeneous/ heterogeneous ± cystic components,
calcifications,
necrotic or hemorrhagic areas ;
- Contrast enhancement features;
- Signs of invasion : infiltration of the fat planes,
invasion of the great mediastinal vessels and pleural involvement (thickening,
nodularity or effusion);
2.
Presence of associated lymphadenopathies ;
3.
CT signs of metastatic disease ;
4.
Other associated lesions -incidentaloma;
5.
Aberrant anatomy/variants.





, undelimited and with compression of the ascending aorta and right pulmonary artery, surrounding the superior vena cava (more than 67% of the circumference). References: Department of Radiology and Medical Imagistics, Fundeni Clinical Institute/ Bucharest 2017")
, heterogeneous, with central necrosis and nodular calcifications, invading the anterior thoracic wall (white arrow), with hypervascular hepatic metastases (arrowhead). References: Department of Radiology and Medical Imagistics, Fundeni Clinical Institute/ Bucharest 2018")
, with central necrosis, without visualization of the left innominate vein and tumor thrombosis at the confluence of the innominate veins (white arrow), including the brachiocephalic artery, left common carotid and subclavian artery, invading the anterior wall of the pulmonary trunk. References: Department of Radiology and Medical Imagistics, Fundeni Clinical Institute/ Bucharest 2010")
, with extension towards the left side of the median line, highly heterogeneous, with central necrotic and hemorrhagic areas (white arrow) and peripheral contrast enhancement, nodular calcifications, hemothorax (arrowhead). References: Department of Radiology and Medical Imagistics, Fundeni Clinical Institute/ Bucharest 2018")
, in contact with the great mediastinal vessels, invading the fat planes, with important mass effect and posterior displacement of the mediastinal vessels, associated lymphadenopathies (white arrow). References: Department of Radiology and Medical Imagistics, Fundeni Clinical Institute/ Bucharest 2011")
 mass (M), originating in the anterior mediastinum, with middle and posterior mediastinum extension, surrounding the great vessels but WITHOUTH invasion, associated bilateral pleurisy (Pl) and pericarditis (P). References: Department of Radiology and Medical Imagistics, Fundeni Clinical Institute/ Bucharest 2018")
, cervical lymphadenopathies. CT aspects: large, well outlined, homogeneous anterior mediastinum mass (M), invading the fat planes adjacent to the great vessels and pericardium, pleural (Pl) and pericardial effusion (P). References: Department of Radiology and Medical Imagistics, Fundeni Clinical Institute/ Bucharest 2017")
. References: Department of Radiology and Medical Imagistics, Fundeni Clinical Institute/ Bucharest 2013")
, right pleural effusion (Pl). References: Department of Radiology and Medical Imagistics, Fundeni Clinical Institute/ Bucharest 2012")
. References: Department of Radiology and Medical Imagistics, Fundeni Clinical Institute/ Bucharest 2017")
 involving the left pulmonary hilum and the anterior mediastinum, nodular calcifications. Histopathologic diagnosis: squamous cell pulmonary carcinoma. References: Department of Radiology and Medical Imagistics, Fundeni Clinical Institute/ Bucharest 2012")
, with extension to the middle mediastinum, left pleural effusion (Pl), associated bone lesions and right chest wall mass (white arrow). References: Department of Radiology and Medical Imagistics, Fundeni Clinical Institute/ Bucharest 2012")

