DISCUSSION
No study to date analyzed the correlation between the RHS and other clinical factors reflecting the underlying immune status of patients,
or the prevalence of the RHS in neutropenic patients affected by pulmonary complications other than IMD.
We therefore compared the clinical and radiological findings for PM and IPA,
and also for non-IMD pulmonary complications,
in patients with hematological malignancy and typical risk factors for IMD (febrile neutropenia and pulmonary infiltrates documented by chest CT),
which is a common but challenging clinical setting in patients undergoing HRCT.
In our study the median time between symptoms and CT scan was 2 days.
All the 23 patients presenting pulmonary infiltrates with the RHS on chest-CT were diagnosed as IMD (23/67; sensibility 34%; specificity 100%; PPV: 1; NPV: 0.48); we didn’t observed the RHS in any of the 41 patients without IMD,
confirming literature about the strict correlation between the RHS and IMD in febrile neutropenic patients.
Regarding the specificity of the RHS for PM,
our study is limited because of the small number of patients,
but we observed that,
of the 4 cases of proven Mucormycosis,
only 2 (50%) showed the reversed halo sign on HRCT imaging,
while of the 11 cases of proven invasive aspergillosis, 4 (36%) showed the RHS.
We didn’t observed the RHS in the only case of Fusariosis,
as reported in literature (Wahba 2008).
Thus,
if we consider only the 17 proven IMD cases,
the RHS has a sensibility and a specificity of 50% and 69%,
respectively,
for the diagnosis of mucormycosis,
and a PPV and NPV of 0.33 and 0.82 respectively.
Of the probable IMD cases,
11/44 (25%) showed the reversed halo sign,
and that’s interesting because the probable cases,
having a positive GM test,
are usually thought to be (and treated as) invasive aspergillosis.
We think those patients could possibly be affected by both Aspergillus and Mucor,
but we can’t prove it.
If we consider the proven and probable IMD cases together (61 patients),
the RHS showed a sensitivity of 50% and a specificity of 74% for the diagnosis of mucormycosis,
with a PPV of 0.118 and a NPV of 0.954,
and a positive and negative likelihood ratio of 1.9 and of 0.67,
respectively.
We observed the RHS in 6 possible IMD cases which responded to antifungal therapy and could probably be mucormycosis,
but we have no mycologic evidence.
In those patients,
the negative results of the GM test would be in accord with a diagnosis of mucormycosis,
but in 4 of them the prophylaxis with posaconazole could also be responsible of the negativity of the GM test.
To note,
4/23 (17%) patients died within 6 days with rapidly enlarging an not cavitating pulmonary lesions.
Taken together,
our results suggest that the presence of the RHS on chest-CT of febrile neutropenic patient is highly suggestive of IMD,
and in the early stage of disease could be indicative of PM,
but it can’t rule out IPA.
Moreover,
the absence of RHS can’t be sufficient to exclude PM,
especially in more advanced stage of disease.
Interestingly,
all the 4 proven Mucormycosis we observed had a positive GM test (the two cases without the RHS had a positive GM test on serum and BAL respectively; the 2 cases with the RHS had both a positive GM test on serum),
but none of them had evidence of a concomitant Aspergillosis at histology.
This result is in contrast with Legouge et al. who,
among 16 proven Mucormycosis,
observed only one patient (6%) with a positive GM test with no evidence of a concomitant aspergillosis.
Again,
the sensibility and specificity of the GM test is a matter of debate.
A recent study (Bourcier 2017) including 27 patients with PM demonstrated that the RHS is more frequently observed in neutropenic patients (78%) than in non neutropenic (31%) but,
to date,
no Authors evaluated its correlation to lymphocytopenia and to disease status.
In our cohort,
we observed the RHS in 23/67 (34%) of patients with IMD,
and it was more frequent in neutropenic patients with active hematology disease status (64%) compared to those with inactive disease.
The association of lymphopenia,
neutropenia and active hematology disease status was more often observed in patients with the RHS (39%) than in patients without the RHS (23%),
but this difference was not significative (p: 0.13).
Thus,
in neutropenic patients with active hematology disease status and pulmonary IMD,
a concomitant lymphocytopenia could play a role in the pathogenesis of the reversed halo sign,
but further evidence are needed to support this hypothesis.
We observed that the RHS lasts for less than 2 weeks in the majority of patients,
but we noted that it lasted for 3-4 weeks in 5/23 (22%) patients and in more than a month in 3/23 (13%) patients.
We noted that the lesions with the RHS may cavitate,
while sometimes they turn into dense nodular lesions (with or without the halo sign) before the cavitation (or air-crescent sign) appears.
Patients with RHS lesions rapidly increasing without cavitation had the worst prognosis (death within a week).
More recently,
Bourcier et al noted that the central area of the RHS showed a reticulation in 87% of patients with PM,
a findings we think it could be associated to pulmonary venous invasion but both studies analyzed CT images acquired without contrast media enhancement.
To our knowledge,
we firstly analyzed the RHS on contrast enhanced CT images.
Indeed,
at our Institution,
it’s a standard practice to submit to CTPA patients with EORTC/MSG possible IMD.
After contrast administration,
20/23 (87%) pulmonary lesion presenting the RHS showed the vessel occlusion sign,
indicative of vascular invasion (figure 3).
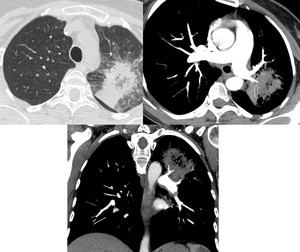
Fig. 3: HRCT finding of pulmonary lesion with the RHS in left upper lobe: the CTPA (oblique and coronal reformatted image) shows the VOS
In the remaining 3 cases,
the VOS was indeterminate because of technical limits of CTPA.
The vessel occlusion sign was appreciable also in 39/44 (89%) of patients with IMD and no-RHS,
and in 1/41 (2%) of patients with diagnosis of no-IMD.
In 5/44 patients of the no RHS-IMD group,
and in 3/41 of the no-IMD group,
the VOS was indeterminate because of technical limits of CTPA (Table 2).
Again,
the VOS seems to be a strong indicator of IMD,
with a sensibility 88.1% specificity 97.6%,
PVV 98.3% ,
NPV 83.3%.
CONCLUSION
Even if our our study is limited,
our findings suggest that the reversed halo sign on CT imaging of neutropenic febrile patients is highly suggestive of IMD,
is more frequently observed in patients with active disease,
neutropenia and lymphocitopenia,
and it’s more frequently associated to pulmonary mucormycosis than to IPA,
but it couldn’t be considered pathognomonic for PM.
Until further well-designed studies are available,
its presence can’t exclude IPA and its absence can’t rule out PM because,
as the well-known halo sign,
it’s a vanishing sign.
By the way,
the presence of the RHS in possible IMD is to be considered suggestive of mucormycosis giving the absence of specific biomarkers,
and can be useful for preemptive initiation of antifungal therapy.
We confirm that the VOS is a strong indicator of IMD,
and is present also in pulmonary lesions with the RHS.
We note that the majority (73%) of patients presenting the reversed halo sign were male.
Our study is limited by its retrospective design and small number of patients,
so it isn’t adequate to draw conclusions about the significance of the RHS in febrile neutropenic patients,
and further studies are advocated.
