Out of 10 patients MRI could accurately reveal Mullerian duct anomalies in all 10 patients.
MRI provides detailed anatomy of both the internal and external uterine cavity.
The maximum no of cases (5) turned out to be bicornuate uterus.
AT MRI: The bicornuate uterus shows a fundal cleft which is greater than 1 cm,
with a soft tissue seperating both the uterine cavities.
This finding helps in differentiating between the bicornuate uterus and uterine didelphys.
Both the uterine horns have normal zonal anatomy.
The appearance of a duplicated cervix (“owl eyes”) is seen in patients with a bicornuate bicollis uterus,
which can be confidently diagnosed in the absence of vaginal duplication.
At USG : The diverged uterine horns and the seperation of the uterine cavities are seen.
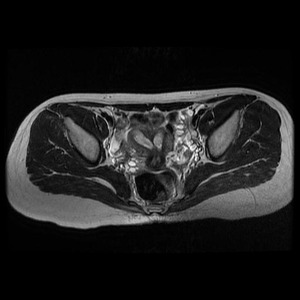
Fig. 1: T2 MRI axial section of the pelvis showing two endometrial cavities, 2 cervix and 2 vaginas - Suggestive of bicornuate bicollis uterus in 18 yr old female.

Fig. 2: Duplex collecting system is noted in the same patient on contrast enhanced ct.
2 patients were diagnosed with Arcuate uterus.
An arcuate uterus occurs with near reabsorption of the uterovaginal septum and is characterized at imaging by a mild indentation of the external fundal contour.
At MRI: There is a normal-sized uterus,
uterine fundal contour is maintained.
There is a broad-based,
smooth prominence of soft tissue at the fundus with indentation of the endometrial cavity.
On T2-weighted images the signal intensity of the soft-tissue is consistent with myometrium without demonstration of fibrous tissue (low signal intensity on T2-weighted images)

Fig. 3: MRI axial section showing sub septate uterus in arcuate a 20 yr old female.
1 patient with Septate uterus
A septate uterus is usually seen in patients with a history of mid-trimester pregnancy loss and is associated with recurrent miscarriages,
hence accurate diagnosis is essential as it is surgically correctable.
At imaging,
the septate uterus is difficult to differentiate it from the bicornuate uterus. The primary difference is the appearance of the uterine fundus; a septate uterus will have a normal convex external fundal contour.
AT USG features suggestive of a septate uterus are interruption of the myometrium by a septum at the fundus .
The fibrous component of the septum is less echogenic relative to myometrium.
Although 3D US may improve assessment of the external uterine contour compared with 2D imaging,
a confident diagnosis is frequently difficult.
The true orthogonal plane to the long axis of the uterus should be used.
A line drawn between the uterine ostia may be used to differentiate between a septate and bicornuate uterus.
In a septate uterus,
the apex of the external fundal contour is more than 5 mm above the interostial line.
By comparison,
in a bicornuate or didelphys uterus,
the apex of the external fundal contour is below or less than 5 mm above the interostial line.
At MR imaging: The uterus is normal in size.
The presence of a clear fundal cleft is a highly reliable indicator for fusion anomalies such as bicornuate uterus rather than reabsorption anomalies (septate or arcuate uterus).
T2-weighted images readily demonstrate the presence of high-signal-intensity myometrium (generally seen closer to the fundus in patients with a complete septum) and a low-signal-intensity fibrous septum,
which may extend to the external cervical os.
1 patient had uterine didelphys it results from complete failure of müllerian duct fusion.
Each duct develops fully with duplication of the uterine horns,
cervix,
and proximal vagina (in three-fourths of patients).
At USG,
In uterus didelphys,
the two uterine horns are widely divergent with separate,
noncommunicating endometrial cavities.
Identification of two cervices and duplicated upper vaginas should be documented.
Duplication of the vagina (hemivaginal septum) may not be apparent; in such circumstances,
the distinction between uterus didelphys and a bicornuate bicollis uterus may be difficult.
AT MR imaging: The two widely divergent uterine horns and two separate cervices are demonstrable. A fundal cleft greater than 1 cm has been reported to be 100% sensitive and specific in differentiation of fusion anomalies (didelphys and bicornuate) from reabsorption anomalies (septate and arcuate).
In uterus didelphys,
the endometrial-to-myometrial ratio as well as the zonal anatomy are normal.
Duplication of the proximal vagina may be visualized at MR imaging,
and this may be further improved by instillation of viscous liquid,
such as ultrasound gel,
into the vagina before imaging.
The presence of a unilateral hemivaginal septum obstructing one of the uterine horns will cause that horn to be markedly distended from blood products,
demonstrating high signal intensity at T1-weighted imaging.
1 patient was diagnosed with hypoplastic uterus.
Early developmental failure of the müllerian ducts results in agenesis or hypoplasia of the proximal two-thirds of the vagina,
cervix,
and uterus.
This anomaly is part of the Mayer-Rokitansky-Küster-Hauser syndrome and this is the most extreme form with complete agenesis of the proximal vagina,
cervix,
and uterus.
Clinical presentation occurs at puberty with primary amenorrhea.
In the setting of isolated partial vaginal agenesis and a normal uterine cavity,
patients may present with primary amenorrhea in conjunction with hematometra or cyclic pelvic pain that may require surgical intervention.
AT USG normal-appearing ovaries with an absent uterus.
However,
a confident diagnosis of uterine agenesis or hypoplasia may be difficult,
especially given that the uterus location is variable.
AT MRI: The ideal choice of investigation for the patient with primary amenorrhea with respect to differentiating uterine hypoplasia or agenesis from other causes of primary amenorrhea.
A further important advantage of MR imaging is the ability to readily evaluate the patient for concurrent renal anomalies,
reported to occur in approximately 40% (30%–50%).
Sagittal T2-weighted sequences are useful in diagnosing of uterine agenesis or hypoplasia,
since the expected location of the vagina,
cervix,
and uterus may be extrapolated from the location of the bladder,
urethra,
and lower vagina.
In the presence of complete uterine agenesis,
there is no identifiable uterus.
A hypoplastic uterus may be seen as a soft-tissue pelvic mass with signal intensity characteristics of normal myometrium (slightly hyperintense on T2-weighted images).
The myometrium of the rudimentary uterus is affected by the presence of circulating female hormones,
and it may even be possible to identify zonal anatomy.



