ECR 2019 / C-2904
Ischemic stroke in vascular territories of the brain
Congress:
ECR 2019
Poster Number:
C-2904
Type:
Educational Exhibit
Keywords:
Ischaemia / Infarction, Imaging sequences, MR-Diffusion/Perfusion, CNS
Authors:
S. Hamid1, S. Hussain2, S. Arooj2; 1Karachi, Sindh/PK, 2Karachi/PK
DOI:
10.26044/ecr2019/C-2904
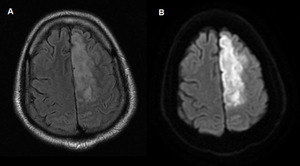
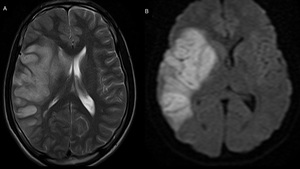
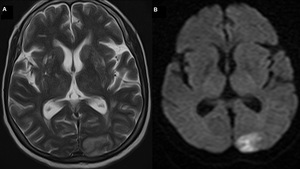
 Axial T2W (B) Axial DWI shows diffusion restricted infarction involving the left paramedian fronto-parietal cerebral cortex corresponding to the territory of the left anterior cerebral artery.")
Fig. 1:
(A) Axial T2W (B) Axial DWI shows diffusion restricted infarction involving the...
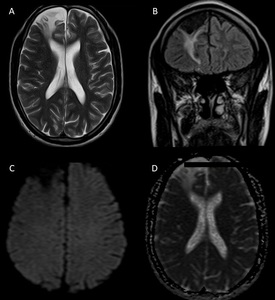
 Axial T2W, (B) Coronal FLAIR, (C) Axial DWI and (D) Axial ADC shows chronic infarction in the right frontal lobe involving the territory of right anterior cerebral artery associated with gliotic and encephalomalacic changes.")
Fig. 2:
(A) Axial T2W, (B) Coronal FLAIR, (C) Axial DWI and (D) Axial ADC shows chronic...
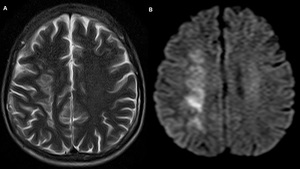
 Axial T2W (B) Axial DWI shows diffusion restricted infarction involving the right fronto-parietal and parietal cortex. Area of involvement corresponds to the deep borderzone and the cortical borderzone area of ACA-MCA and MCA-PCA territories.")
Fig. 3:
(A) Axial T2W (B) Axial DWI shows diffusion restricted infarction involving the...
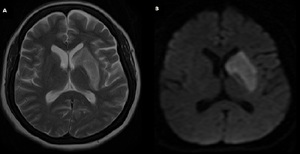
 Axial T2W (B) Coronal T2W (C) Axial DWI and (A) Axial ADC shows acute infarction involving the putamen and head and body of the right caudate nucleus. There is also involvement of the posterior limb of internal capsule. Findings correspond to the territory of the medial and lateral lenticulostriate branches of the ACA and MCA.")
Fig. 4:
(A) Axial T2W (B) Coronal T2W (C) Axial DWI and (A) Axial ADC shows acute...
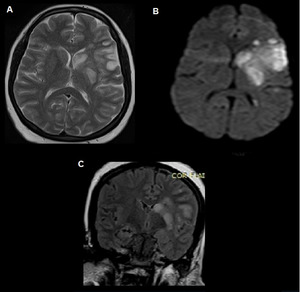
 Axial T2W (B) Axial DWI shows acute infarction involving the head and body of caudate nucleaus and putamen of the left basal ganglia corresponding to the territory of the lateral and medial lenticulostriate branches of the ACA and MCA.")
Fig. 5:
(A) Axial T2W (B) Axial DWI shows acute infarction involving the head and body...
 Axial T2W MR brain shows infarction involving left frontal lobe anterior to the sylvian fissure. Area of involvement corresponds to the territory of the superior division of the left middle cerebral artery.")
Fig. 6:
(A,B) Axial T2W MR brain shows infarction involving left frontal lobe anterior...
 Axial T2W (B) Coronal T2W (C) Axial DWI and (D) Axial ADC shows large area of infarction involving the left perisylvian cerebral cortex and the insular cortex. Basal ganglia appears spared. Findings correspond to the territory of the superior and inferior divisions of the left middle cerebral artery.")
Fig. 7:
(A) Axial T2W (B) Coronal T2W (C) Axial DWI and (D) Axial ADC shows large area...
 Axial T2W (B) Axial DWI shows a large area of infarction involving the left perisylvian cerebral cortex, adjacent insular cortex, head of caudate and putamen of the left basal ganglia. Findings represent infarction involving the territory of the left MCA proximal main stem (superior division, inferior division and lenticulostriate branches).")
Fig. 8:
(A) Axial T2W (B) Axial DWI shows a large area of infarction involving the left...
 Axial T2W and (B) Axial DWI shows infarction of the left antero-inferior temporal lobe corresponding to the territory of the inferior division of the left middle cerebral artery.")
Fig. 9:
(A) Axial T2W and (B) Axial DWI shows infarction of the left antero-inferior...
 Axial T2W (B) Axial DWI (C) Coronal T2W shows a diffusion restricted area of infarction involving the left perisylvian cerebral cortex, adjacent insular cortex. In addition there is involvement of the head of caudate and putamen of the left basal ganglia. Findings correspond to the territory of the deep cortical branches, deep penetrating branches and the lenticulostraite branches of left MCA.")
Fig. 10:
(A) Axial T2W (B) Axial DWI (C) Coronal T2W shows a diffusion restricted area...
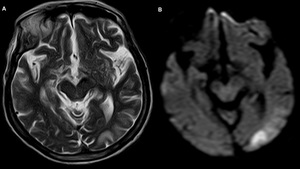
 Axial (B) Axial DWI shows a wedge-shaped cortical based area of infarction involving the left occipital lobe corresponding to the territory of the left posterior cerebral artery.")
Fig. 11:
(A) Axial (B) Axial DWI shows a wedge-shaped cortical based area of infarction...
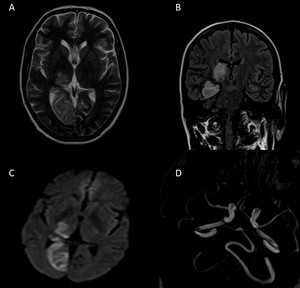
 Axial T2W, (B) Coronal FLAIR, (C) Axial DWI shows diffusion restricted infarction involving the right thalamus, right medial occipital and medial temporal lobes. Area of involvement corresponds to the territory of the right proximal posterior cerebral artery. (D) MRA image shows occlusion of the right PCA.")
Fig. 12:
(A) Axial T2W, (B) Coronal FLAIR, (C) Axial DWI shows diffusion restricted...
 Axial (B) Axial DWI shows an area of cortical based infarction involving parasagittal left occipital lobe corresponding to the territory of the left posterior cerebral artery.")
Fig. 13:
(A) Axial (B) Axial DWI shows an area of cortical based infarction involving...
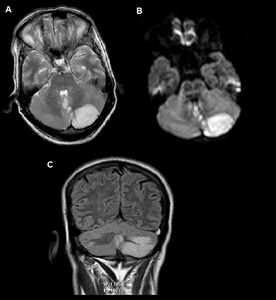
 Axial T2W and (B) Axial DWI and (C) Coronal T2W MR brain shows an area of infarction involving the caudal portion of the left cerebellar hemisphere corresponding to the territory of right posterior inferior cerebellar artery (PICA).")
Fig. 14:
(A) Axial T2W and (B) Axial DWI and (C) Coronal T2W MR brain shows an area of...
 Axial T2W and (B) Axial DWI MRI brain shows infarction involving the right cerebellar hemisphere and lateral medulla corresponding to the territory of right posterior inferior cerebellar artery.")
Fig. 15:
(A) Axial T2W and (B) Axial DWI MRI brain shows infarction involving the right...
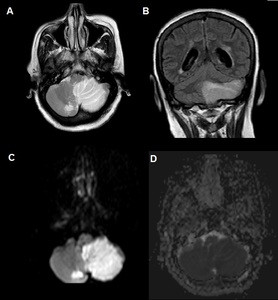
 Axial T2W (B) Coronal T2W (C) Axial DWI and (D) Axial ADC shows an area of infarction involving the inferior cerebellum, inferior cerebellar vermis and lateral medulla corresponding to the territory of left posterior inferior cerebellar artery (PICA). Small area of infarction was also seen in the contralateral cerebellum.")
Fig. 16:
(A) Axial T2W (B) Coronal T2W (C) Axial DWI and (D) Axial ADC shows an area of...
 Axial T2W and (B) Axial DWI shows focal area of infarction involving the territory of the perforating branches of right sided anterior and posterior inferior cerebellar arteries (AICA and PICA).")
Fig. 17:
(A) Axial T2W and (B) Axial DWI shows focal area of infarction involving the...
 Axial and (B) Axial DWI shows an area of acute ischemic infarction involving the right thalamus corresponding to the territory of the tuberothalamic artery.")
Fig. 18:
(A) Axial and (B) Axial DWI shows an area of acute ischemic infarction...
 Axial and (B) Axial DWI shows an area of acute ischemic infarction involving the posterior limb of the right internal capsule representing lacunar infarct caused by occlusion of the small perforating branches of ACA and MCA or anterior choroidal artery.")
Fig. 19:
(A) Axial and (B) Axial DWI shows an area of acute ischemic infarction...
 Axial FLAIR at the level the thalamus shows bilateral paramedian thalamic infarcts (B) Axial FLAIR at the level of the midbrain demonstrate bilateral midbrain infarcts with characteristic V-sign of hyperintense signal intensity along the pial surface of the interpeduncular fossa. Findings corresponds to the territory of Artery of Percheron. References: Lazzaro NA et al. Artery of Percheron Infarction: Imaging Patterns and Clinical Spectrum .AJNR Am J Neuroradiol 31:1283– 89.")
Fig. 20:
(A) Axial FLAIR at the level the thalamus shows bilateral paramedian thalamic...
 Axial FLAIR at the level the thalamus shows bilateral paramedian thalamic infarcts (B) Axial FLAIR at the level of the midbrain demonstrate bilateral midbrain infarcts with characteristic V-sign of hyperintense signals along the pial surface of the interpeduncular fossa. Findings represent acute ischemic infarction involving the territory of the Artery of Percheron. References: Lazzaro NA et al. Artery of Percheron Infarction: Imaging Patterns and Clinical Spectrum .AJNR Am J Neuroradiol 31:1283– 89.")
Fig. 21:
(A) Axial FLAIR at the level the thalamus shows bilateral paramedian thalamic...