ECR 2019 / C-3656
Differential diagnosis of intracranial ring-enhancing lesions: a practical approach
Congress:
ECR 2019
Poster Number:
C-3656
Type:
Educational Exhibit
Keywords:
Contrast agent-intravenous, Diagnostic procedure, MR-Spectroscopy, MR, CT, Oncology, Neuroradiology brain, CNS, Education, Infection, Neoplasia, Inflammation
Authors:
A. Manzella, D. Sousa, M. Vasconcelos, L. ďż˝. Neto, E. Cavalcante, S. Morais, G. Lago, L. Nascimento-Neto; Recife/BR
DOI:
10.26044/ecr2019/C-3656
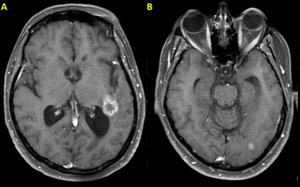
 and (B) demonstrate metastatic deposits, the largest lesion with ring-enhancement adjacent to the left posterior horn of the lateral ventricle.")
Fig. 12:
Brain metastases in a 41-year-old woman with ovarian tumor. Axial post-contrast...
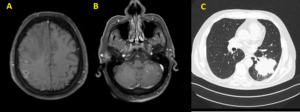
 as well as nodular lesions (B). Chest CT images (C) demonstrate a large spiculated mass in the left lung.")
Fig. 13:
Brain metastases in a 60-year-old man with lung cancer. Axial MR images show...
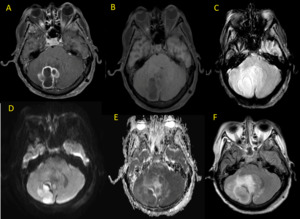
 and (B) with central restricted diffusion (C-F)")
Fig. 14:
Multiple abscesses in a 2 year-old child. Axial MR images show oval...
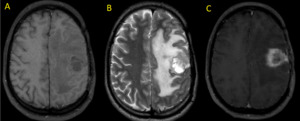
 T1 and (B) T2 show a parietal heterogeneous mass with extensive perilesional edema. T1 post-contrast image (C) demonstrates ring enhancement with thick irregular wall and a shaggy inner margin.")
Fig. 19:
GBM. Axial MR Images (A) T1 and (B) T2 show a parietal heterogeneous mass with ...
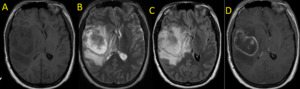
 T1, (B) T2 and (C) FLAIR show a large mass with heterogeneous content and perilesional edema. T1 post-contrast weighted image (D) reveals ring-enhancement with irregular wall.")
Fig. 20:
GBM. Axial MR Images. (A) T1, (B) T2 and (C) FLAIR show a large mass with...
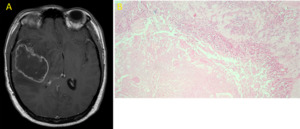
 and microscopy (B) show a pseudopalisade sign.")
Fig. 21:
Glioblastoma. T1 post-contrast MR Image (A) and microscopy (B) show a...
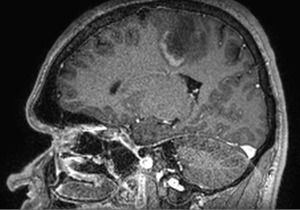
 T1 pre-contrast (B) FLAIR and (C) T1 post-contrast show a frontal lobe mass with intense vasogenic edema producing midline shift. The lesion crosses the midline (butterfly sign).")
Fig. 22:
MR images (A) T1 pre-contrast (B) FLAIR and (C) T1 post-contrast show a frontal...
 Coronal T2 MRI.")
Fig. 23:
Butterfly sign in a pacient with glioblastoma. (A) Coronal T2 MRI.
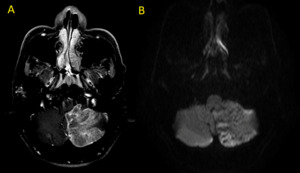
 T1 post-contrast and (B) diffusion axial MR images. Note Irregular ring-enhancement in A.")
Fig. 25:
Patient with posterior fossa infarct. (A) T1 post-contrast and (B) diffusion...
 FLAIR and (B) post-contrast T1. Oval lesion with ring enhacement is seen on the right. Also note perilesional edema.")
Fig. 26:
Patient with a history of head trauma. Axial MR Images (A) FLAIR and (B)...
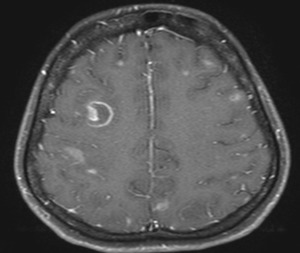
 FLAIR and (B) T1 post-contrast axial MR images demonstrate multiple small lesions with ring enhancement. Surrounding edema is seen in A.")
Fig. 27:
Tuberculomas. (A) FLAIR and (B) T1 post-contrast axial MR images demonstrate...

Fig. 28:
Neutoxoplasmosis. Axial T1 post-contrast MR image shows ring enhancing lesion...
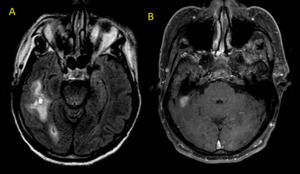
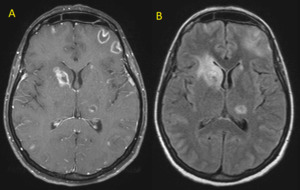
 and axial FLAIR (B) show the eccentric target sign which is highly suggestive of this infection.")
Fig. 29:
Neurotoxoplasmosis. Axial T1 post-contrast MR Image (A) and axial FLAIR (B)...
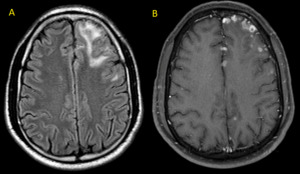
 sagittal DIR, (B) sagittal FLAIR, (C) axial FLAIR and (D) axial post-contrast T1. Dawson’s fingers is best seen in sagittal images. Also note enhancement of some of these lesions.")
Fig. 32:
Multiple hyperintense lesions in a patient with multiple sclerosis. (A)...
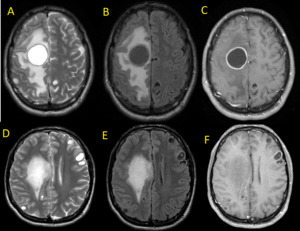
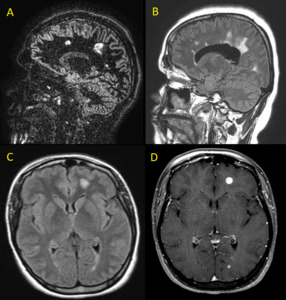
 FLAIR, (B) diffusion, (C) ADC map and (D) T1 post-contrast demonstrate a ring-enhancing lesion with surrounding edema and peripheral restricted diffusion. Note the incomplete ring sign which is highly suggestive of demyelination.")
Fig. 33:
Multiple sclerosis. Axial MR images (A) FLAIR, (B) diffusion, (C) ADC map and...
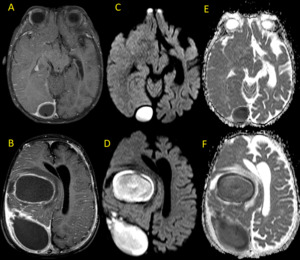
 T2, (B, E) FLAIR and (C, F) T1 post-contrast reveal cystic lesions with ring-enhancement, the largest one with surrounding edema.")
Fig. 35:
Neurocysticercosis. Axial MR images (A, D) T2, (B, E) FLAIR and (C, F) T1...

Fig. 37:
Schematic drawings. Ring-enhancing lesions.

Fig. 34:
Multiple sclerosis. Multivoxel MR spectroscopy. Ring-enhancing lesion in the...

Fig. 15:
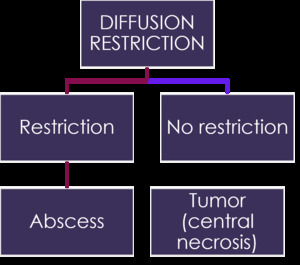
Summary and take home message. Diffusion.

Fig. 16:
Summary and take home message.

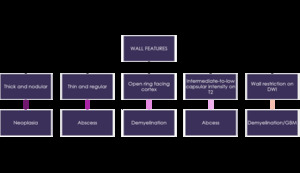
Fig. 17:
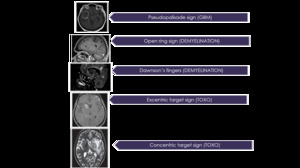
Summary and take home message. Typical signs.

Fig. 24:
GBM. MR multivoxel spectroscopy. Note reduced NAA and elevated choline peak in...
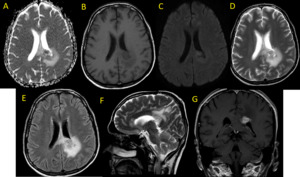
 show ring-enhancing mass with vasogenic edema on the left involving the corpus callosum and crossing the midline.")
Fig. 30:
Primary Lymphoma. Multiplanar MR images (A-G) show ring-enhancing mass with...