How we implemented the service.
MRI Radiographers at a large tertiary MRI centre recieved in-house training from a clinical physicist and specialised radiographer supported by a Neuro-Radiologists with experience in the field.
Training included identifying patients who could benefit from ASL during pre-screening checks,
how to perform ASL techniques and how to optimise patient position to ensure diagnostic scans.
After a period of training and support,
radiographers were able to run the service with little input from neuroradiologists and supporting staff.
During a 10 month period,
104 consecutive patients with gliomas,
undergoing diagnostic MRI at 3 Tesla on a Philips Achieva or Philips Ingenia,
underwent an extended protocol that included pseudocontinuous ASL (pcASL).
ASL-PWI maps scanner generated and archived together with conventional imaging were produced with out any additional time added to the radiographers schedule.
The extended protocol initially added 10 minutes to the original booking time,
however after conventional sequences were optimised this was no longer necessary.
A qualitive retrospective survey completed by radiographers demonstrated that 90% of radiographers felt either confident or very confident in performing the ASL technique and were happy in independantant protocol selection.
100% of the PWI maps reviewed were considered diagnostic quality.
Evaluation of the ASL-PWI maps in reporting.
A sub-group of patients with available follow up imaging (n=39: 20 glioblastoma multiforme,
15 astrocytoma,
4 oligodendroglioma) were selected for futher analysis to examine the usefulness of the scanner produced ASL-PWI maps.
Two observers examined images and concluded RANO scores in two parts: conventional images alone and conventional imaging with ASL-PWI.
Confidence was measured using Likert scales 1-5 (1,
very unconfident to 5,
very confident) and differences compared.
Lastly,
all diagnoses were checked against follow up imaging.
A statistically significant increase in average confidence levels was observed for inclusion of ASL (4.44 SD 0.8)) compared to conventional imaging alone (4.02 (SD 0.65)).
Below is an example of a case which demonstrates how ASL with conventional imaging increases confidence.
Case:
A 43 year old male diagnosed with an anaplastic astrocytoma WHO grade III in the left temporal region who underwent a surgical excision. The ASL-PWI,
shown in figure 2., demonstrates increased signal relating to increased cerebral blood flow in the remnant left hippocampal and left parahippocampal gyrus which shows less convincing enhancement on the post contrast T1 weighted images.
This was decided to be residual disease.
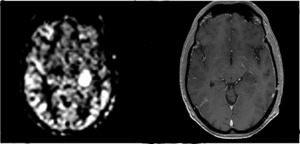
Fig. 2: ASL-PWI and Post contrast T1 weighted images showing increased cerebral blood flow to the left parahippocampal region.
The enhancing areas of the left lateral surgical margin,
as seen in figure 3.,
showed no ASL-PWI hyperintensity and was considered changes due to treatment.
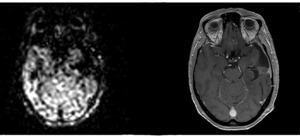
Fig. 3: ASL-PWI and post contrast T1 weighted images of the left lateral surgical margin.
Following this scan the patient received adjuvant therapy.



