ECR 2020 / C-00807
Has the significance of incidental findings on unenhanced CT KUB for urolithiasis been underestimated? A retrospective study of over 2500 patients
Congress:
ECR 2020
Poster Number:
C-00807
Type:
Scientific Exhibit
Keywords:
Performed at one institution, Cross-sectional study, Retrospective, Inflammation, Calcifications / Calculi, Acute, Diagnostic procedure, Computer Applications-General, Colonography CT, CT-High Resolution, CT-Enterography, CT, Kidney, Emergency, Abdomen, Abdominal Viscera
Authors:
U. S. Umer, S. Alam, A. N. Khan, S. G. Ghaus, M. Abdullah, A. Nawaz, M. Asif, N. Gul; Peshawar/PK
DOI:
10.26044/ecr2020/C-00807
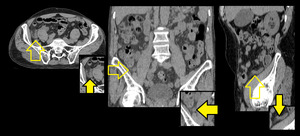
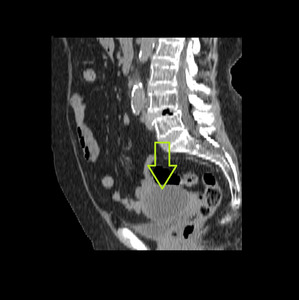
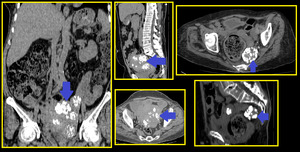
. Fluid filled distended appendix is seen in right iliac fossa with periappendiceal fat stranding (better appreciated on sagittal image) and minimal free fluid (better seen on axial image). It is important to compare both iliac fossa, when in doubt. The clue here is the increased diameter of appendix alongwith surrounding soft tissue haze.")
Fig. 1:
CT KUB in a patient with right flank pain. Axial and reformatted images...

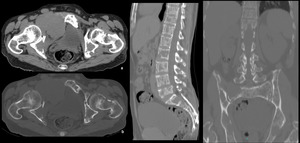
Fig. 10:
Extensive Bone lesions. Multiplanar reformatted images of a patient with pain...
Bone window images reveal multiple sclerotic lesions in bones. Increased bone density can even be appreciated in soft tissue window (a) and a soft tissue mass seen in right iliac region, which appears to be nodal metastases. Such generalized bone sclerosis has differentials of metastatic CA prostate or bone marrow infiltrative disease and requires further work up. Umbilical hernia noted on sagittal image (c)")
Fig. 11:
Extensive sclerotic bone lesions. Multiplanar CT images in a patient with...
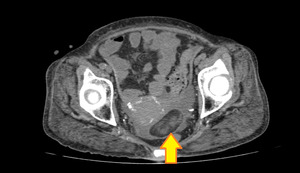
 and enlarged uterus for the age of patient. Such finding can be due to cervical stenosis and further workup should be done concerning cervical malignancy.Degenerative spine changes are seen with background osteopenia, even appreciated without bone window.Few atheromatous calcifications noted in abdominal aorta.")
Fig. 8:
Sagittal reformatted image of CT KUB showing fluid distended endometrial cavity...

Fig. 3:
Ovarian Dermoid with possible Torsion diagnosed on CT KUB in an elderly female...

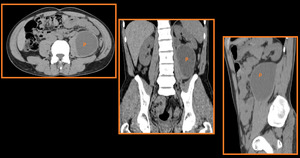
Fig. 12:
Axial and coronal reformatted images showing incidental finding of right...
 if such finding is encountered as incidental finding.")
Fig. 14:
Colonic Diverticulosis. Multiple non-inflamed colonic diverticulae seen in...
 and few subserosal in location.The calcification in fibroids is patchy and often called as popcorn-like in appearance.")
Fig. 13:
Calcified fibroids. Multiple CT images of different patients showing calcified...

Fig. 15:
Cholelithiasis. CT KUB done for flank pain showing incidental finding of small...

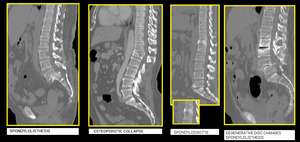
Fig. 18:
Spine related incidental findings like spondylolisthesis, spondylolysis,...

Fig. 16:
Inguinal Hernia. Sagittal reformatted image showing right inguinal hernia...

Fig. 7:
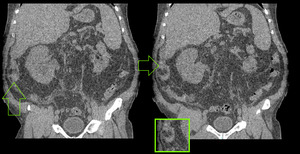
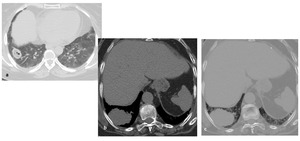
Liver lesions. Axial CT images in apatient with pain in bilateral flanks....
 Upper image shows a consolidating opacity in right lower lobe with atoll sign (inner low attenuation surrounded by high attenuation) suggesting possibility of organizing pneumonia, however detailed chest evaluation should be done in such cases for confirmation and extent of disease process.
(b & c) Another patient's CT images in both lung and soft tissue window showing a large mass in right lower lobe. This requires further workup with detailed chest evaluation and biopsy should be done.")
Fig. 9:
Incidental lung finding in visualized lower sections of chest.
(a) Upper...

Fig. 2:
Subhepatic Appendicitis diagnosed on CT KUB in a patient with pain in right...

Fig. 4:
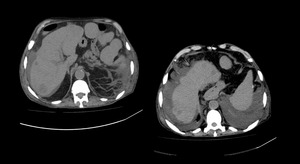
Large left Psoas abscess. Axial and reformatted sections of CT KUB showing...

Fig. 6:
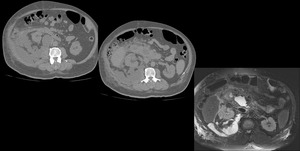
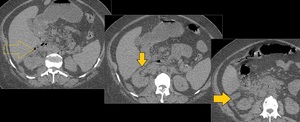
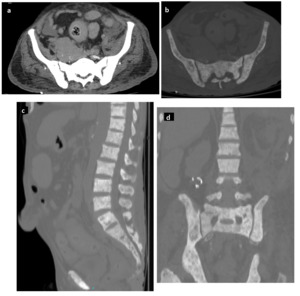
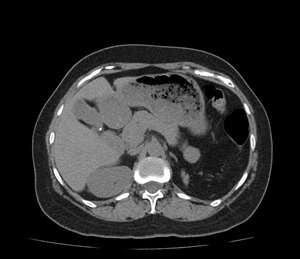
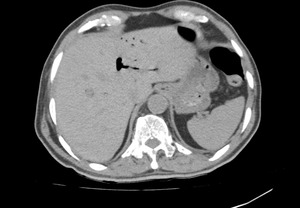
Duodenal Perforation. Axial CT images showing small air and fluid loculations...
 showing multiple retroperitoneal fluid collections along right perinephric fascia, pancreatic head and duodenum.The possible differentials here included pancreatitis with pseudocysts and retroperitoneal perforation of bowel. Latter was confirmed with MRI seen in the lower most image, where a defect is clearly visualized in the medial wall of second part of duodenum.")
Fig. 5:
Duodenal Perforation. Axial CT KUB images (upper two images) showing multiple...

Fig. 17:
Pneumobilia. CT KUB done for renal colic. Incidental finding of air in biliary...
.")
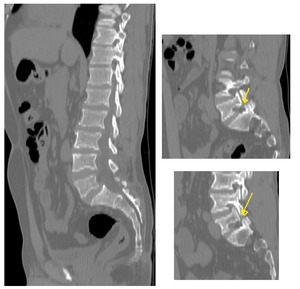
Fig. 19:
Fractured bilateral pars inter articularis. Sagittal reformatted images showing...

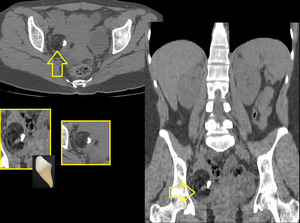
Fig. 20:
Incidental finding of sclerosis in left iliac bone with thickening underlying...