TECHNICAL SPECIFICATIONS OF IMAGE DATA ACQUISITION
PI-RADS v2.1 presents some updates on technical specifications of image data acquisition:
- recommended T2-weighted (T2W) imaging planes to be performed;
- clarification of b-values to use for purposes of diffusion-weighted imaging (DWI) acquisition and apparent diffusion coefficient (ADC) map calculation;
- advice about dynamic contrast-enhanced (DCE) temporal resolution and preferred imaging sequence.
T2-weighted images
PI-RADS version 2 (v2) stated multiplanar (axial, coronal, and sagittal) T2W images are usually obtained. Instead, PI-RADS v2.1 recommends that T2W images should always be obtained in the axial plane (either straight axial to the patient or in an oblique axial plane matching the long axis of the prostate) and a minimum of one additional orthogonal plane (sagittal and/or coronal), reflecting the important role of T2 signal intensity and morphology evaluation, including lesion encapsulation, in PI-RADS assessment, which can be limited by partial volume averaging when viewing in only one plane.
Diffusion-weighted images
PI-RADS v2 advised the use of a low b-value between 50 and 100 sec/mm2 for the generation of ADC maps, but it was found to be technically more challenging than the use of a minimum b-value of 0 sec/mm2 for some magnetic resonance (MR) systems, and, likely, perfusion effects do not substantively impact clinical interpretation of DWI. That is why PI-RADS v2.1 now recommends using one low b-value set at 0-100 sec/mm2, maintaining a second (intermediate) b-value set at 800-1000 sec/mm2, and optional additional b-values between 100 and 1000 sec/mm2 that may provide more accurate ADC calculations and estimations of extrapolated high b-value images (≥1400 sec/mm2). Furthermore, a high b-value (≥1,400 sec/mm2) image set still mandatory and, for PI-RADS v2.1, preferably should be obtained from a separate acquisition rather than calculated from the low and intermediate b-value images.
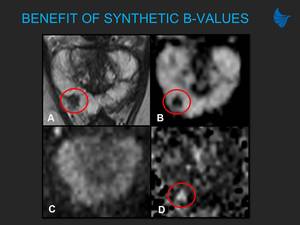
Fig. 2: Benefit of synthetic b-values in a 62-year-old biopsy-naive man with a PSA of 5.2 ng/ml. (A, B) Axial T2-weighted image (A) shows an area of low signal in the right mid-gland, with restricted diffusion on ADC maps (B). (C) Acquired large field of view (FOV) b=1,000 image shows no clear area with increased signal. (D) Synthetic b=1,500 image calculated from large FOV b=50/500/1,000 image shows reduced signal in the normal prostate with increased signal of the lesion, confirming PI-RADS score 4 for DWI (markedly restricted diffusion). Targeted transperineal biopsy showed Gleason 3+4.
Dynamic contrast-enhanced images
The PI-RADS v2 suggested temporal resolution of 10 seconds (<7 seconds preferred) is updated to ≤15 seconds in PI-RADS v2.1, based on studies that have not shown any added diagnostic benefit from high temporal resolution imaging, and the potential to result in important compromises in image quality, including spatial resolution.
Furthermore, PI-RADS v2 stated either a 2D or 3D T1-weighted (T1W) gradient echo (GRE) sequence may be used, although 3D is preferred, while for PI-RADS v2.1 3D T1W GRE is recommended, as it is generally available using modern systems.
INTERPRETATION CRITERIA
PI-RADS v2.1 presents updates and clarifications in interpretation criteria:
- further description of assessment of lesions in central zone (CZ) and anterior fibromuscular stroma (AFMS);
- revision in criteria for T2W imaging scores of 1 and 2 in transition zone (TZ);
- revision in determination of overall assessment category in TZ;
- revisions in criteria for DWI scores of 2 and 3;
- clarification of the distinction between positive and negative enhancement on DCE;
- clarification in measurement of the prostate volume;
- revision in sector map.
Lesions in central zone and anterior fibromuscular stroma
Lesions occasionally appear to originate in the CZ or involve the AFMS. Asymmetry on T2WI, high b-value image, or ADC, as well as focal early enhancement, may help differentiate tumors from benign anatomy. Since PCa does not originate in the AFMS, when reporting a suspicious lesion in the AFMS, criteria for either the PZ or the TZ should be applied, depending on the zone from which the lesion appears most likely to be originating.
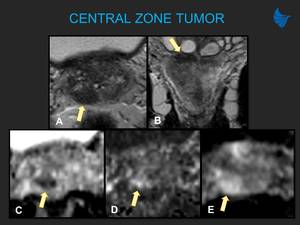
Fig. 3: CZ tumor (yellow arrows) in a 48-year-old patient with a rising PSA and familiar history of prostate cancer. Asymmetry between the central zone of the prostate, with lower signal intensity on T2W on the right side (A – axial, B – coronal), and restricted diffusion within this area (C, D), presenting early contrast enhancement (E). Reported as undetermined finding, suggesting intermediate probability for clinically significant cancer (PI-RADS 3). Biopsy of this region showed Gleason 3+4 disease.
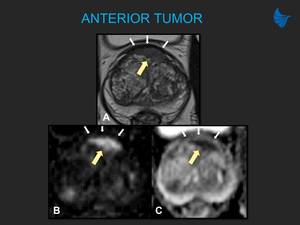
Fig. 4: Anterior tumor in a 78-year-old man with a PSA of 11.6 ng/ml. Lenticular lesion in anterior TZ (yellow arrows) bulging the AFMS, measuring 2.3 cm, presenting a homogeneous and intermediate T2W signal (A), with marked restricted diffusion (B, C), suggesting a very high probability for clinically significant neoplasia (PI-RADS 5). Targeted biopsy confirmed Gleason 4+3 tumor. AFMS (white arrows) shows markedly hypointense signal on T2W along the anterior aspect of the prostate, hypointense signal similar to that of the background prostate on b = 1,500, and signal similar to that of the background prostate on ADC map. Note that lesions do not originate from the AFMS, but can arise from the adjacent PZ or TZ, or invade into the AFMS.
Revision in criteria for T2W imaging scores of 1 and 2 in transition zone
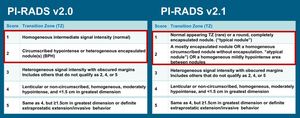
Table 1: Comparison of assessment for T2W in TZ (changes highlighted in red).
References: PI-RADS Steering Committee
Predominant imaging characteristics of the background and similar-appearing findings scattered throughout the TZ should not be scored. The shape and margin features of TZ findings should be assessed in at least two planes on T2W images. Typical benign prostatic hyperplasia (BPH) nodules (round, circumscribed, and completely encapsulated on T2W) were assigned a T2W score of 2 in PI-RADS v2, but now in PI-RADS v2.1 receive a score of 1, that is, considered a normal variant and do not have to be reported separately.
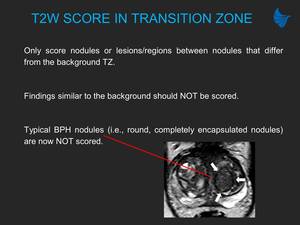
Fig. 5: New PI-RADS T2W imaging category 1 in the TZ. Fully encapsulated nodule in the left TZ (arrows) is of PI-RADS category 1 (previously, version 2 = category 2). Additional benign features include foci of high T2 signal within, consistent with microcysts (dilated hyperplastic acini), and posteriorly location. T2W imaging is the dominant sequence in the TZ; overall PI-RADS score 1.
Mostly encapsulated nodule, a homogeneous circumscribed nodule without encapsulation, or a homogeneous mildly hypointense area between nodules receive a T2W score of 2.
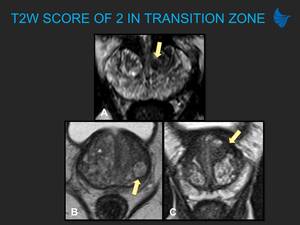
Fig. 6: PI-RADS T2W imaging category 2 in the TZ. (A) A homogeneous circumscribed nodule without encapsulation (“atypical nodule”) OR (B) a mostly encapsulated nodule OR (C) a homogeneous mildly hypointense area between nodules. T2W imaging is the dominant sequence in the TZ; overall PI-RADS score 2.
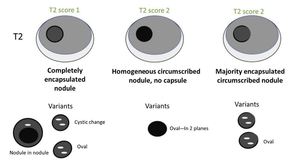
Fig. 7: Schematic diagram summarizing the updated definitions of T2W scores of 1 and 2 in the TZ. Assessment of nodule shape and margins should be done in at least two planes. Oval or spherical shape and cystic change are acceptable features within nodules.
References: Turkbey B, Rosenkrantz AB, Haider MA, Padhani AR, Villeirs G, Macura KJ, Tempany CM, Choyke PL, Cornud F, Margolis DJ, Thoeny HC, Verma S, Barentsz J, Weinreb JC. Prostate Imaging Reporting and Data System Version 2.1: 2019 Update of Prostate Imaging Reporting and Data System Version 2. Eur Urol. 2019. pii: S0302-2838(19)30180-0
Revision in determination of overall assessment category in transition zone
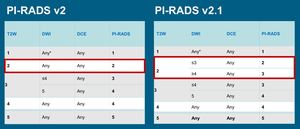
Table 2: Comparison of overall assessment category in TZ (change highlighted in red).
References: PI-RADS Steering Committee
DWI characteristics have been incorporated for atypical nodules in TZ in PI-RADS v2.1. Thus, focal findings with a T2W score of 2 are upgraded to assessment category 3 if they have a DWI score >4 (i.e., markedly restricted diffusion).
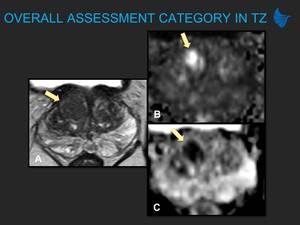
Fig. 8: Up-scoring T2 category 2 lesion with DWI in an 82-year-old biopsy-naive man with a PSA of 11.0 ng/ml. (A) Partly encapsulated homogeneous circumscribed nodule within the right anterior basal TZ, PI-RADS score 2 on T2W imaging. (B, C) The nodule demonstrates marked restricted diffusion on b=1,500 (B) and ADC maps (C), PI-RADS score 4 on DWI. Overall PI-RADS v2.1 score 3. Targeted transperineal biopsy demonstrated Gleason 3+4 tumor.
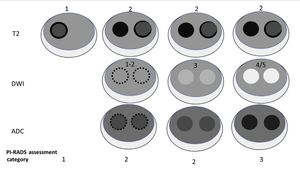
Fig. 9: Schematic diagram summarizing the updated overall assessment category in TZ incorporating DWI. A partially encapsulated or circumscribed, unencapsulated nodule with clearly restricted diffusion (DWI score 4 or 5) is scored a 3 (dotted lines indicate the region of a near isointense lesion where the borders are indistinct or difficult to define because of the near isointensity).
References: Turkbey B, Rosenkrantz AB, Haider MA, Padhani AR, Villeirs G, Macura KJ, Tempany CM, Choyke PL, Cornud F, Margolis DJ, Thoeny HC, Verma S, Barentsz J, Weinreb JC. Prostate Imaging Reporting and Data System Version 2.1: 2019 Update of Prostate Imaging Reporting and Data System Version 2. Eur Urol. 2019. pii: S0302-2838(19)30180-0
Revisions in criteria for DWI scores of 2 and 3
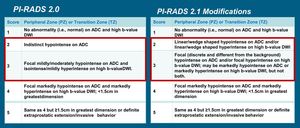
Table 3: Comparison of DWI scores (changes highlighted in red).
References: PI-RADS Steering Committee
PI-RADS v2 had problematic definitions for DWI scores of 2 and 3. In the revision of the DWI score 2 criteria, the term “indistinct” was replaced by “linear/wedge-shaped”, and it was added that the lesion may be, besides hyperintense on ADC, hyperintense on DWI, decreasing common errors of interpretation.
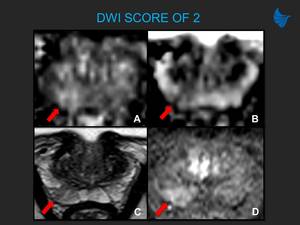
Fig. 10: New DWI category 2 in a 52-year-old patient, with a palpable nodule in the right base of prostate and a PSA of 1.6 ng/ml. (A, B) Wedge-shaped area of mild hyperintensity on b=1,500 (A) and mild hypointensity on ADC (B). PI-RADS version 2 this would be category 3 due to “Focal mildly/moderately hypointense on ADC and isointense/mildly hyperintense on high b-value DWI”; however, on v2.1 this is category 2 due to “linear/wedge-shaped area hypointense on ADC and/or hyperintense on high b-value DWI”. (C, D) T2W shows a wedge-shaped area of low signal (C) with positive DCE due to focal early enhancement matching a T2/DWI abnormality (D). DWI is the dominant sequence in the PZ, therefore the overall assessment category is PI-RADS 4 using v2, but PI-RADS score 2 with v2.1. Targeted biopsy was benign, with histological features of inflammation.
In reviewing the criteria for DWI scores of 3-5, the terms "focal" (“discrete and different from the background”), and "marked" (“a more pronounced signal change than any other focus in the same zone”) are better defined. It is established that, in score 3, the lesion may be markedly hypointense on ADC or markedly hyperintense on high b-value DWI, but not both. These changes provide more detailed definitions for DWI score 3 and reduce overdiagnosed lesions as category 4.
Clarification of the distinction between positive and negative enhancement on DCE
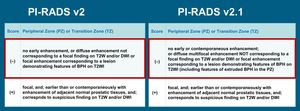
Table 4: Comparison of DCE scores (change highlighted in red).
References: PI-RADS Steering Committee
In PI-RADS v2, the features that constituted a negative DCE score and assessment of widespread multifocal enhancement are unclear. In PI-RADS v2.1, “diffuse multifocal enhancement NOT corresponding to a focal finding on T2W” is considered negative score on DCE.
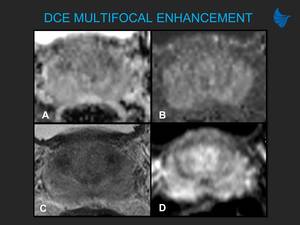
Fig. 11: Diffuse multifocal enhancement in a 50-year-old man with a PSA of 2.6 ng/ml. (A, B) No clear area with restricted diffusion is seen. (C, D) PZ presents slightly diffuse T2 signal heterogeneity (C), with early and diffuse multifocal contrast enhancement, that is, negative score on DCE (D), suggesting probable prostatitis. This patient was treated with antibiotics, presenting regression of these findings.
Clarification in measurement of the prostate volume
The PI-RADS v2 recommendation to report prostate volume using ellipsoid formulation remains, but PI-RADS v2.1 advises to measure maximum anteroposterior diameter on midsagittal T2W instead of axial T2W.
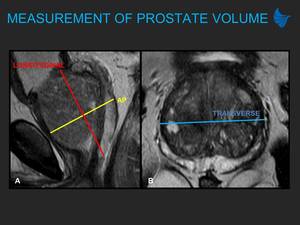
Fig. 12: Measurements for ellipsoid formula when calculating prostate volume according to PI-RADS v2.1. (A, B) Maximum longitudinal diameter and maximum AP diameter should be measured on midsagittal T2W (A), whereas maximum transverse diameter should be measured on axial T2W (B). In the exemplified case, if the maximum AP diameter were measured on axial T2W, as recommended by PI-RADS v2, there would be a false increase of 18% in prostate volume.
Revision in sector map
In PI-RADS v2.1, the revised sector map contains two additional sectors in the base PZ: right and left medial posterior PZ, amounting to a total of 41 sectors.
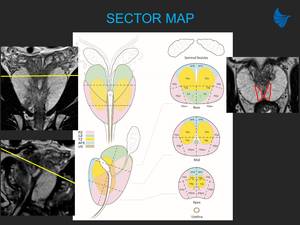
Fig. 13: Correspondence between sector map diagram and MRI images. PI-RADS v2.1 sector map contains two additional sectors for the right and left posterior medial PZ (PZpm) at the base (highlighted in red). There are now 41 sectors in total (38 for prostate, 2 for the seminal vesicles, 1 for the membranous urethra).
References: The prostate sector diagram in: Turkbey B, Rosenkrantz AB, Haider MA, Padhani AR, Villeirs G, Macura KJ, Tempany CM, Choyke PL, Cornud F, Margolis DJ, Thoeny HC, Verma S, Barentsz J, Weinreb JC. Prostate Imaging Reporting and Data System Version 2.1: 2019 Update of Prostate Imaging Reporting and Data System Version 2. Eur Urol. 2019. pii: S0302-2838(19)30180-0. MRI images from Department of Radiology, Hospital Moinhos de Vento. Porto Alegre, Brazil.
ROLE OF DYNAMIC CONTRAST-ENHANCED IMAGING
DCE MRI has a very limited role in PI-RADS v2.1: when positive, elevate a finding in the PZ with a DWI score of 3 to an assessment category of 4. There would be many potential benefits in performing prostate MRI without DCE (bpMRI), such as elimination of adverse events and gadolinium retention that have been associated with some gadolinium-based contrast agents, shortened examination time, and reduced costs.
However, in some studies, DCE MRI has been reported to improve the sensitivity of prostate mpMRI, assisting in detection of csPCa in both the PZ and TZ. Additionally, in clinical practice, some have viewed DCE as a “safety-net” or “back-up” sequence, especially when DWI is degraded by artifacts or inadequate signal-to-noise ratio (SNR), what PI-RADS Steering Committee take into account to continue recommending DCE MRI.
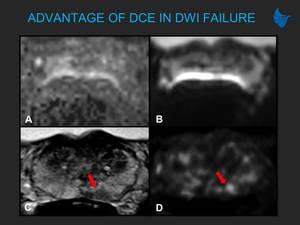
Fig. 17: Advantage of DCE in DWI failure in a 51-year-old man with a PSA of 5.35 ng/ml. (A, B) Distortion artifact due to rectal gas affects b-value (A) and ADC maps (B) making these uninterpretable. (C) Lesion with low T2 signal in the left PZ. (D) Focal early enhancement within the area makes this suspicious for tumor. Biopsy showed Gleason 3+4 disease.
There is no specific recommendation for use of bpMRI. PI-RADS continues to recommend mpMRI, especially when:
- clinical risk factors indicate the likely presence of significant disease that should not be missed (e.g., family history, prior negative biopsy, active surveillance, risk calculator);
- prior negative bpMRI at persistent suspicion;
- technical factors leading to suboptimal image quality of DWI.
When bpMRI is performed and DCE data are not obtained:
- TZ assessment remains unchanged;
- assessment category for a finding in the PZ remains primarily based on the DWI score, and the lesions with a score of 3 on DWI will not be upgraded.
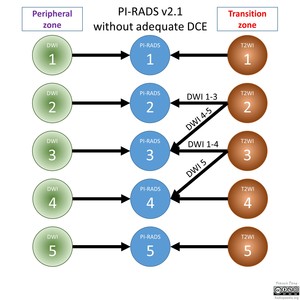
Fig. 15: PI-RADS v2.1 flowchart if DCE inadequate or not obtained (bpMRI).
References: Courtesy of Dr Francis Deng, Radiopaedia.org, rID: 70893


 Axial T2-weighted image (A) shows an area of low signal in the right mid-gland, with restricted diffusion on ADC maps (B). (C) Acquired large field of view (FOV) b=1,000 image shows no clear area with increased signal. (D) Synthetic b=1,500 image calculated from large FOV b=50/500/1,000 image shows reduced signal in the normal prostate with increased signal of the lesion, confirming PI-RADS score 4 for DWI (markedly restricted diffusion). Targeted transperineal biopsy showed Gleason 3+4.")
 in a 48-year-old patient with a rising PSA and familiar history of prostate cancer. Asymmetry between the central zone of the prostate, with lower signal intensity on T2W on the right side (A – axial, B – coronal), and restricted diffusion within this area (C, D), presenting early contrast enhancement (E). Reported as undetermined finding, suggesting intermediate probability for clinically significant cancer (PI-RADS 3). Biopsy of this region showed Gleason 3+4 disease.")
 bulging the AFMS, measuring 2.3 cm, presenting a homogeneous and intermediate T2W signal (A), with marked restricted diffusion (B, C), suggesting a very high probability for clinically significant neoplasia (PI-RADS 5). Targeted biopsy confirmed Gleason 4+3 tumor. AFMS (white arrows) shows markedly hypointense signal on T2W along the anterior aspect of the prostate, hypointense signal similar to that of the background prostate on b = 1,500, and signal similar to that of the background prostate on ADC map. Note that lesions do not originate from the AFMS, but can arise from the adjacent PZ or TZ, or invade into the AFMS.")
.
References: PI-RADS Steering Committee")
 is of PI-RADS category 1 (previously, version 2 = category 2). Additional benign features include foci of high T2 signal within, consistent with microcysts (dilated hyperplastic acini), and posteriorly location. T2W imaging is the dominant sequence in the TZ; overall PI-RADS score 1.")
 A homogeneous circumscribed nodule without encapsulation (“atypical nodule”) OR (B) a mostly encapsulated nodule OR (C) a homogeneous mildly hypointense area between nodules. T2W imaging is the dominant sequence in the TZ; overall PI-RADS score 2.")
30180-0")
.
References: PI-RADS Steering Committee")
 Partly encapsulated homogeneous circumscribed nodule within the right anterior basal TZ, PI-RADS score 2 on T2W imaging. (B, C) The nodule demonstrates marked restricted diffusion on b=1,500 (B) and ADC maps (C), PI-RADS score 4 on DWI. Overall PI-RADS v2.1 score 3. Targeted transperineal biopsy demonstrated Gleason 3+4 tumor.")
 is scored a 3 (dotted lines indicate the region of a near isointense lesion where the borders are indistinct or difficult to define because of the near isointensity).
References: Turkbey B, Rosenkrantz AB, Haider MA, Padhani AR, Villeirs G, Macura KJ, Tempany CM, Choyke PL, Cornud F, Margolis DJ, Thoeny HC, Verma S, Barentsz J, Weinreb JC. Prostate Imaging Reporting and Data System Version 2.1: 2019 Update of Prostate Imaging Reporting and Data System Version 2. Eur Urol. 2019. pii: S0302-2838(19)30180-0")
.
References: PI-RADS Steering Committee")
 Wedge-shaped area of mild hyperintensity on b=1,500 (A) and mild hypointensity on ADC (B). PI-RADS version 2 this would be category 3 due to “Focal mildly/moderately hypointense on ADC and isointense/mildly hyperintense on high b-value DWI”; however, on v2.1 this is category 2 due to “linear/wedge-shaped area hypointense on ADC and/or hyperintense on high b-value DWI”. (C, D) T2W shows a wedge-shaped area of low signal (C) with positive DCE due to focal early enhancement matching a T2/DWI abnormality (D). DWI is the dominant sequence in the PZ, therefore the overall assessment category is PI-RADS 4 using v2, but PI-RADS score 2 with v2.1. Targeted biopsy was benign, with histological features of inflammation.")
.
References: PI-RADS Steering Committee")
 No clear area with restricted diffusion is seen. (C, D) PZ presents slightly diffuse T2 signal heterogeneity (C), with early and diffuse multifocal contrast enhancement, that is, negative score on DCE (D), suggesting probable prostatitis. This patient was treated with antibiotics, presenting regression of these findings.")
 Maximum longitudinal diameter and maximum AP diameter should be measured on midsagittal T2W (A), whereas maximum transverse diameter should be measured on axial T2W (B). In the exemplified case, if the maximum AP diameter were measured on axial T2W, as recommended by PI-RADS v2, there would be a false increase of 18% in prostate volume.")
 at the base (highlighted in red). There are now 41 sectors in total (38 for prostate, 2 for the seminal vesicles, 1 for the membranous urethra).
References: The prostate sector diagram in: Turkbey B, Rosenkrantz AB, Haider MA, Padhani AR, Villeirs G, Macura KJ, Tempany CM, Choyke PL, Cornud F, Margolis DJ, Thoeny HC, Verma S, Barentsz J, Weinreb JC. Prostate Imaging Reporting and Data System Version 2.1: 2019 Update of Prostate Imaging Reporting and Data System Version 2. Eur Urol. 2019. pii: S0302-2838(19)30180-0. MRI images from Department of Radiology, Hospital Moinhos de Vento. Porto Alegre, Brazil.")

.
References: Courtesy of Dr Francis Deng, Radiopaedia.org, rID: 70893")

 Distortion artifact due to rectal gas affects b-value (A) and ADC maps (B) making these uninterpretable. (C) Lesion with low T2 signal in the left PZ. (D) Focal early enhancement within the area makes this suspicious for tumor. Biopsy showed Gleason 3+4 disease.")