ECR 2020 / C-04512
High-value multidetector CT angiography for diagnosis of acute mesenteric ischemia.
Congress:
ECR 2020
Poster Number:
C-04512
Type:
Educational Exhibit
Keywords:
Performed at one institution, Not applicable, Retrospective, Acute, Diagnostic procedure, CT-Angiography, Catheter arteriography, Interventional vascular, Gastrointestinal tract, Emergency, Emergency Imaging
Authors:
S. Brugger1, R. M. Piqueras Olmeda1, M. Ballesta2, P. Estelles Lerga1; 1Valencia/ES, 2VALENCIA, Valencia/ES
DOI:
10.26044/ecr2020/C-04512

Fig. 1:
Causes of vascular insuffiency.

Fig. 2

Fig. 3

Fig. 4:
Pathophysiology of intestinal ischemia

Fig. 5:
American College of Radiology . ACR Appropiateness criteria Imaging of AMI

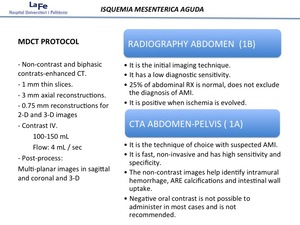
Fig. 6:
CT protocol

Fig. 7:
Most frequent locations of stenosis according to etiology.

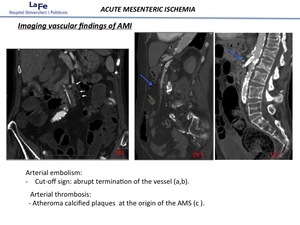
Fig. 8:
Vascular imaging findings

Fig. 9:
Bowel imaging findings

Fig. 10:
Bowel imaging findings

Fig. 11

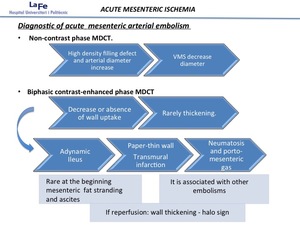
Fig. 12:
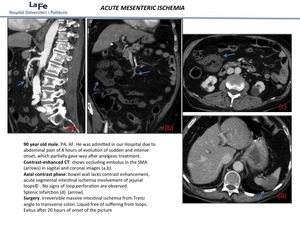
Mesenteric arterial embolism

Fig. 13:
Mesenteric arterial embolism

Fig. 14

Fig. 15

Fig. 16:
Mesenteric arterial thrombosis

Fig. 17

Fig. 18

Fig. 19:
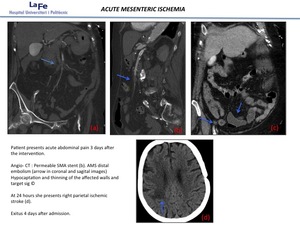
Mesenteric venous thrombosis

Fig. 20

Fig. 21:
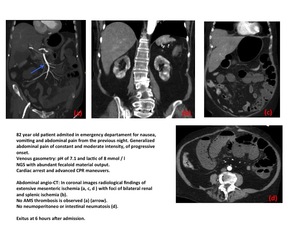
Nonoclusive mesenteric ichemia

Fig. 22:
Nonocclusive mesneteric ischemia

Fig. 23

Fig. 24

Fig. 25

Fig. 26

Fig. 27

Fig. 28

Fig. 29