Protocol and imaging technique of whole body MRI
Institutional Review Board approval and informed consent from all patients performed 1.5T and 3T whole body MRI with CS-VIBE were obtained.
Whole body MRI was performed at 1.5T and 3.0T MR system with 48 or 64 independent receiver channels and a total imaging matrix system.
Prior to the examination, a 22 gauge intravenous catheter was placed into an antecubital vein of arm to facilitate contrast medium injection. No bowel preparation, air insufflation, or intravenous antispasmodic agents were used.
Detailed parameters for whole-body imaging sequences are provided in Fig 2.
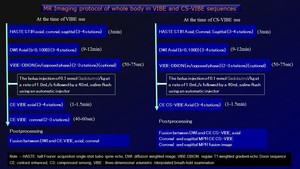
Fig. 2: MR Imaging protocol of whole body in VIBE and CS-VIBE sequences.
Whole-body DWIs were performed in three of four stations (chest, abdomen, pelvis) in the axial plane using a single-shot spin-echo echo-planar imaging (EPI) sequence and b-value of 0,1000s/mm2. Parallel 2 imaging was performed with a generalized autocalibrating partially parallel acquisitions (GRAPPA) algorithm (12, 13). For the acquisition of the whole body, free breathing was performed.
Protocol of high spatial resolution contrast-enhanced 3D VIBE on the compressed sensing technique (CS-VIBE)(WIP)
CS-VIBE was acquired in three or four stations (chest, abdomen, pelvis) in the axial plane with thin slices and 18 seconds breath-holding after the bolus injection of 0.1 mmol/kg gadobutrol at a rate of 1.0mL, followed by 40mL of saline flush using an automatic injector.
Detailed parameters for whole-body CS-VIBE sequence is provided in Table 1.
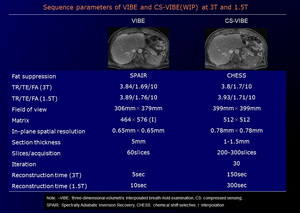
Table 1: Sequence parameters of VIBE and CS-VIBE (WIP) at 3T and 1.5T.
After data acquisition, the whole body entire DWI and CS-VIBE images were composed in axial plane from each station. Furthermore, fusion images between DWI and CS-VIBE (CS-FDWI) were reconstructed in axial, coronal and sagittal planes using commercially available workstation with a fusion algorithm (Fig 3).
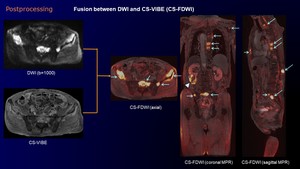
Fig. 3: Postprocessing of fusion imaging between DWI and CS-VIBE (CS-FDWI).
Postprocessing CS-FDWI and MPR images reveal multiple high signal bone metastases (arrows) in the sternum, left scapula, vertebral bodies and pelvic bones. Coronal MPR image on CS-FDWI shows heterogeneous high intensity RCC (arrowhead).
Advantages of CS-VIBE (9-11)
1. Higher spatial resolution image
2. Lower partial volume effect
3. Possibility of reconstruction with high spatial resolution in all planes (Fig 4)
4. Possibility of fusion reconstructed imaging with high spatial resolution
Disadvantages of CS-VIBE
1. A large amount of reconstruction time
2. Necessity of high-performance reconstructed machine
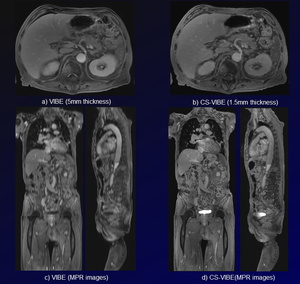
Fig. 4: Comparison of VIBE and CS-VIBE.
Axial images on both VIBE and CS-VIVE (a, b) is nearly same quality. However, CS- VIBE is superior to VIBE on MPR images (c, d).
Pictorial review of whole body CS-FDWI
Detection of primary and metastatic lesions using CF-FDWI
1. Rectal cancer (Fig 5)
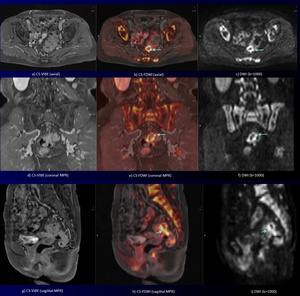
Fig. 5: A 70-year-old woman with rectal cancer.
CS-VIBE and MPR images (a, d, g) show detail anatomy.
CS-FDWI (b, e, h) and DWI (c, f, i) reveal an annular high signal intensity rectal cancer with perirectal tissue invasion (arrows).
2. Gastric gastrointestinal stromal tumor (GIST) and descending colon cancer (Fig 6)
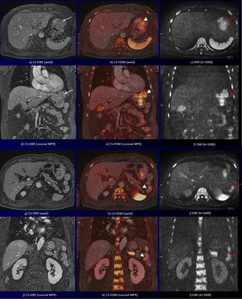
Fig. 6: A 65-year-old man with gastric gastrointestinal stromal tumor (GIST) and descending colon cancer.
CS-VIBE and coronal MPR CS-VIBE (a, d) show a heterogeneous enhancing tumor with lobulated margin at the gastric anterior wall (white arrows). DWI and coronal MPR DWI (c, f) show a high intensity tumor without sufficient anatomical information (red arrows). Corresponding CS-FDWI and MPR CS-VIBE (b, e) show a high intensity GIST with sufficient anatomical information, which was proved at the partial gastrectomy (arrowheads).
CS-VIBE and coronal MPR CS-VIBE (g, j) show detail anatomical information, however, it is difficult to detect a descending colon cancer.
DWI and coronal MPR DWI (i, l) show a high intensity tumor without sufficient anatomical information (arrows). Corresponding CS-FDWI and MPR CS-VIBE (h, k) show a high intensity descending colon cancer with sufficient anatomical information (arrowheads).
3. Renal pelvic transitional cell cancer with multiple lung and lymph node metastases (Fig 7)
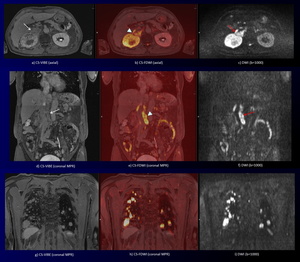
Fig. 7: Right renal pelvic transitional cell cancer with multiple lung and lymph node metastases in a 66-year-old man.
CS-VIBE (a) shows a heterogeneous enhancing tumor in the right renal hilum
with renal cortical invasion and dilated renal pelvis (white arrow).
Corresponding DWI (b) shows a high intensity tumor (red arrows). Furthermore, corresponding CS-FDWI (b) shows a high intensity renal pelvic transitional cell cancer, which was confirmed at biopsy, with sufficient anatomical information (arrowhead). Coronal MPR CS-VIBE (d) shows heterogeneous enhancing lymphadenopathy at aortocaval space (white arrow).
Corresponding coronal MPR DWI (e) shows high intensity lymphadenopathy (red arrow). Furthermore, corresponding MPR CS-FDWI (e) reveals high intensity lymph node metastases with sufficient anatomical information (arrowhead). MPR CS-VIBE (g) shows multiple homogeneous enhancing pulmonary nodules.
Corresponding coronal MPR CS-FDWI (h, i) and DWI show multiple high intensity lung metastases.
Surveillance of therapy using CF-FDWI
1. Recurrent lesion of rectal cancer during chemotherapy (Fig 8)
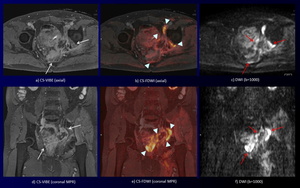
Fig. 8: A 60-year-old man with recurrent lesion of rectal cancer.
DWI and coronal MPR DWI (c, f) show an irregular-shaped high intensity mass (red arrows) without sufficient anatomical information.
CS-VIBE and coronal MPR CS-VIBE (a, d) reveal an irregular-shaped heterogeneous enhancing mass (white arrows) without definite tumor extent.
Furthermore, CS-FDWI and coronal MPR CS-VIBE show improved conspicuity of the irregular-shaped high signal intensity mass (recurrent lesion of rectal cancer) with muscle and ischium invasion and definite tumor extent (arrowheads) .
2. Recurrent multiple lymph node metastases of ureteral cancer after right nephrectomy and ureterectomy during chemotherapy (Fig 9)
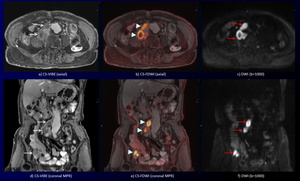
Fig. 9: A 75-year-old woman with recurrent multiple lymph node metastases of ureteral cancer after right nephrectomy and ureterectomy.
DWI and coronal MPR DWI (c, f) show multiple high intensity lymphadenopathy without sufficient anatomical information (red arrows).
CS-VIBE and coronal MPR CS-VIBE (a, d) reveal multiple heterogeneous enhancing lymphadenopathy with sufficient anatomical information (white arrows). Furthermore, CS-FDWI and coronal MPR CS-VIBE show improved conspicuity of the multiple high signal intensity lymphadenopathy with sufficient anatomical information (arrowheads).
3. Gastric cancer with multiple lymph node, hepatic and bone metastases (Fig 10)
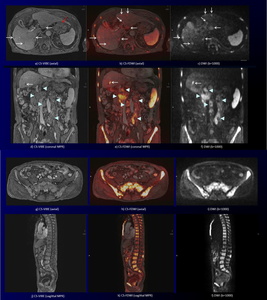
Fig. 10: A 75-year-old man with gastric ca. with multiple lymph node, hepatic and bone metastases during chemotherapy.
CS-VIBE and coronal MPR images (a, d) reveal multiple small low signal intensity nodules in the liver (white arrows) and heterogeneous enhancing lymphadenopathy (arrowheads). Gastric cancer at the cardia is thickening with heterogeneous enhancement on CS-VIBE (red arrow).
DWI and coronal MPR images (c, f) show multiple high intensity nodules in the liver (white arrows) and heterogeneous high signal lymphadenopathy (arrowheads). Gastric lesion on DWI is not identified due to cardiac movement. CS-FDWI and coronal MPR images (b, e) show improved conspicuity of multiple liver (white arrows) and lymph node (arrowheads) metastases with sufficient anatomical information. CS-VIBE and coronal MPR images (g, j) reveal multiple enhancing bone metastases in the sternum, whole vertebral bodies and pelvic bones with sufficient anatomical information.
Corresponding DWI and CS-FDWI (h, I, k, l) shows multiple high signal bone metastases.
4. Lung cancer with multiple bone metastases (Fig 11)
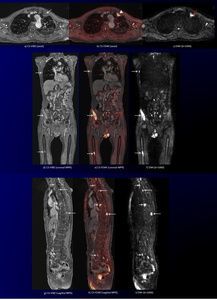
Fig. 11: Left lung cancer with multiple bone metastases during chemotherapy in a 78-year-old man.
CS-VIBE (a) shows an irregular-shaped enhancing tumor in the left lung (white arrow). Corresponding DWI (c) shows a high intensity tumor (red arrow). Corresponding CS-FDWI (b) reveals a high intensity lung cancer, representing viable lesion, with sufficient anatomical information (arrowhead). Coronal and sagittal MPR CS-VIBE images (d, g) reveal multiple enhancing bone metastases in the right rib, right ilium, right femur and vertebral bodies with sufficient anatomical information (white arrows).
Corresponding DWI and CS-FDWI (e, f, h, i) show improved conspicuity of multiple high signal bone metastases (white arrows).
5. Prostate cancer with multiple bone metastases during hormonal therapy. (Fig 12)
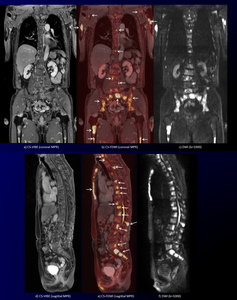
Fig. 12: Prostate cancer with multiple bone metastases during hormonal therapy in a 75-year-old man.
Coronal and sagittal MPR CS-VIBE images (a, d) reveal multiple enhancing bone metastases. Corresponding DWI (c, f) show multiple high signal bone metastases. Corresponding coronal and sagittal MPR CS-FDWIs show improved conspicuity of multiple bone metastases in the sternum, vertebral bodies, pelvic bones, bilateral humerus, scapula, and femur with sufficient anatomical information (arrows).
6. Breast cancer with multiple bone metastases during hormonal therapy. (Fig 13)
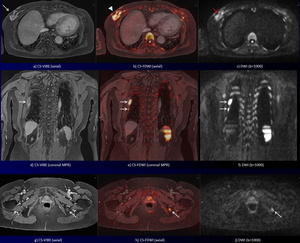
Fig. 13: Right breast cancer with multiple bone metastases during hormonal therapy in a 77-year-old woman.
CS-VIBE (a) shows an irregular-shaped enhancing tumor in the right breast (white arrow). Corresponding DWI (c) shows a high signal intensity tumor (red arrows). Corresponding CS-FDWI (b) reveals a high signal intensity breast cancer in the right breast with sufficient anatomical information (arrowhead). CS-VIBE and coronal MPR images (d, g) reveal some enhancing bone metastases (arrows). Corresponding DWI (f, j) show high signal bone metastases (arrows). Corresponding CS-FDWI and coronal MPR images show improved conspicuity of bone metastases in the right ribs and left ischium with sufficient anatomical information (arrows).



 at 3T and 1.5T.")
.
Postprocessing CS-FDWI and MPR images reveal multiple high signal bone metastases (arrows) in the sternum, left scapula, vertebral bodies and pelvic bones. Coronal MPR image on CS-FDWI shows heterogeneous high intensity RCC (arrowhead).")
 is nearly same quality. However, CS- VIBE is superior to VIBE on MPR images (c, d).")
 show detail anatomy.
CS-FDWI (b, e, h) and DWI (c, f, i) reveal an annular high signal intensity rectal cancer with perirectal tissue invasion (arrows).")
 and descending colon cancer.
CS-VIBE and coronal MPR CS-VIBE (a, d) show a heterogeneous enhancing tumor with lobulated margin at the gastric anterior wall (white arrows). DWI and coronal MPR DWI (c, f) show a high intensity tumor without sufficient anatomical information (red arrows). Corresponding CS-FDWI and MPR CS-VIBE (b, e) show a high intensity GIST with sufficient anatomical information, which was proved at the partial gastrectomy (arrowheads).
CS-VIBE and coronal MPR CS-VIBE (g, j) show detail anatomical information, however, it is difficult to detect a descending colon cancer.
DWI and coronal MPR DWI (i, l) show a high intensity tumor without sufficient anatomical information (arrows). Corresponding CS-FDWI and MPR CS-VIBE (h, k) show a high intensity descending colon cancer with sufficient anatomical information (arrowheads).")
 shows a heterogeneous enhancing tumor in the right renal hilum
with renal cortical invasion and dilated renal pelvis (white arrow).
Corresponding DWI (b) shows a high intensity tumor (red arrows). Furthermore, corresponding CS-FDWI (b) shows a high intensity renal pelvic transitional cell cancer, which was confirmed at biopsy, with sufficient anatomical information (arrowhead). Coronal MPR CS-VIBE (d) shows heterogeneous enhancing lymphadenopathy at aortocaval space (white arrow).
Corresponding coronal MPR DWI (e) shows high intensity lymphadenopathy (red arrow). Furthermore, corresponding MPR CS-FDWI (e) reveals high intensity lymph node metastases with sufficient anatomical information (arrowhead). MPR CS-VIBE (g) shows multiple homogeneous enhancing pulmonary nodules.
Corresponding coronal MPR CS-FDWI (h, i) and DWI show multiple high intensity lung metastases.")
 show an irregular-shaped high intensity mass (red arrows) without sufficient anatomical information.
CS-VIBE and coronal MPR CS-VIBE (a, d) reveal an irregular-shaped heterogeneous enhancing mass (white arrows) without definite tumor extent.
Furthermore, CS-FDWI and coronal MPR CS-VIBE show improved conspicuity of the irregular-shaped high signal intensity mass (recurrent lesion of rectal cancer) with muscle and ischium invasion and definite tumor extent (arrowheads) .")
 show multiple high intensity lymphadenopathy without sufficient anatomical information (red arrows).
CS-VIBE and coronal MPR CS-VIBE (a, d) reveal multiple heterogeneous enhancing lymphadenopathy with sufficient anatomical information (white arrows). Furthermore, CS-FDWI and coronal MPR CS-VIBE show improved conspicuity of the multiple high signal intensity lymphadenopathy with sufficient anatomical information (arrowheads).")
 reveal multiple small low signal intensity nodules in the liver (white arrows) and heterogeneous enhancing lymphadenopathy (arrowheads). Gastric cancer at the cardia is thickening with heterogeneous enhancement on CS-VIBE (red arrow).
DWI and coronal MPR images (c, f) show multiple high intensity nodules in the liver (white arrows) and heterogeneous high signal lymphadenopathy (arrowheads). Gastric lesion on DWI is not identified due to cardiac movement. CS-FDWI and coronal MPR images (b, e) show improved conspicuity of multiple liver (white arrows) and lymph node (arrowheads) metastases with sufficient anatomical information. CS-VIBE and coronal MPR images (g, j) reveal multiple enhancing bone metastases in the sternum, whole vertebral bodies and pelvic bones with sufficient anatomical information.
Corresponding DWI and CS-FDWI (h, I, k, l) shows multiple high signal bone metastases.")
 shows an irregular-shaped enhancing tumor in the left lung (white arrow). Corresponding DWI (c) shows a high intensity tumor (red arrow). Corresponding CS-FDWI (b) reveals a high intensity lung cancer, representing viable lesion, with sufficient anatomical information (arrowhead). Coronal and sagittal MPR CS-VIBE images (d, g) reveal multiple enhancing bone metastases in the right rib, right ilium, right femur and vertebral bodies with sufficient anatomical information (white arrows).
Corresponding DWI and CS-FDWI (e, f, h, i) show improved conspicuity of multiple high signal bone metastases (white arrows).")
 reveal multiple enhancing bone metastases. Corresponding DWI (c, f) show multiple high signal bone metastases. Corresponding coronal and sagittal MPR CS-FDWIs show improved conspicuity of multiple bone metastases in the sternum, vertebral bodies, pelvic bones, bilateral humerus, scapula, and femur with sufficient anatomical information (arrows).")
 shows an irregular-shaped enhancing tumor in the right breast (white arrow). Corresponding DWI (c) shows a high signal intensity tumor (red arrows). Corresponding CS-FDWI (b) reveals a high signal intensity breast cancer in the right breast with sufficient anatomical information (arrowhead). CS-VIBE and coronal MPR images (d, g) reveal some enhancing bone metastases (arrows). Corresponding DWI (f, j) show high signal bone metastases (arrows). Corresponding CS-FDWI and coronal MPR images show improved conspicuity of bone metastases in the right ribs and left ischium with sufficient anatomical information (arrows).")