Type:
Educational Exhibit
Keywords:
Performed at one institution, Diagnostic or prognostic study, Retrospective, Metastases, Cancer, Imaging sequences, MR-Diffusion/Perfusion, MR, Oncology, Liver, Bones, Oncologic Imaging
Authors:
H. Horikoshi1, A. Okayama1, T. kawakami1, N. Oya1, T. Akiyoshi1, K. Maruyama2, M. Nickel3; 1Ota/JP, 2Tokyo/JP, 3Erlangen/DE
DOI:
10.26044/ecr2020/C-08171
Background
The accurate detection of metastatic and recurrent lesions for cancer patients play an important role in clinical care. Imaging is fundamental to evaluation and management of cancer patients. While CT and PET are well established imaging modalities for cancer and lymphoma, the number of serial examinations required throughout the course of therapy and subsequent surveillance has prompted concern regarding cumulative ionizing radiation exposure(1).
Whole-body MRI, by enabling wide field-of-view imaging with high spatial and contrast resolution to provide robust soft-tissue characterization in the absence of ionizing radiation, has emerged as a viable oncologic imaging technique. On whole MRI examinations, coronal acquisition is standard for most sequences owing to reduced imaging time, although axial images are variably added for some sequences (2-8). Especially, contrast-enhanced 3D volume-interpolated breath-hold examination (VIBE) is a useful addition for target evaluation. However, the slice thickness of VIBE for whole body MRI is thick and prevents multiplanar reconstruction.
Compressed sensing (CS) is a recent technique to increase speed of acquisition of MR images on the sparsity, incoherent sampling and reconstruction algorithm (9-11). A compressed sensing (CS)-VIBE sequence (Work in Progressive: WIP) that improved through plane and thickness spatial resolution (less than 1.5mm) allows multiplanar reconstruction and assessment of morphologic lesion characteristics in multiple planes (Fig 1).
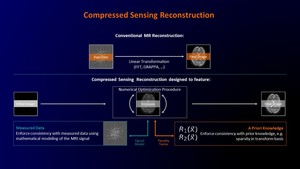
Fig. 1: Sequence diagram for a compressed sensing reconstruction.
Courtesy of Dominik Nickel, Ph.D. Siemens Healthcare GmbH
Diffusion weighted imaging (DWI) can evaluate the diffusion capacity of water molecules and detect pathologic region with restricted-water molecules by malignant tumor cells. Therefore, whole body DWI may be
of value in detection of metastatic lesions. However, a limitation of DWI is its suppression of background body signals, as a result of which sufficient anatomical information is lacking (12,13). On the other hand, fusion imaging between DWI and 3D CS-VIBE is able to show both metastatic lesions and detail anatomical information. The aim of this presentation is to describe whole body high spatial resolution contrast enhanced CS-VIBE imaging and fusion imaging between DWI and CS VIBE for the detection of metastatic lesions.

