Renal Carcinoma Mimics → A diagnosis problem
*Normal anatomical variants in the kidney can mimic renal masses
*We cannot always distinguish benign tumors from cancers
*Diagnostic errors and unnecessary biopsy or nephrectomy in some conditions
*Many benign tumor are resected…
*Imaging and biopsy not fully utilized when a mass suspected of being cancer is detected…
*Radiologist’s goals → Detection + Imaging Features and Differential Diagnosis + Recommendations = Management → Follow-up
The steps in the differentiation of a renal lesion on CT/MRI are:
Step 1: Know clinical history of the patient, clinical and paraclinical characteristics at the moment of presentation, and if ultrasonography of the abdomen or other imaging modality has been performed previously
Step 2: Know the basic CT and MRI protocols needed in evaluation of renal masses

Fig. 1: CT protocol
References: Fig. 1 CT protocol Department of Radiology, Cluj County Emergency Hospital, Romania 2020

Fig. 2: MRI protocol
References: Department of Radiology, Cluj County Emergency Hospital, Romania 2020
Step 3: The first step in order to distinguish renal pseudolesions is to know the renal anatomy and its CT/MRI correlation

Fig. 3: This image allows to differentiate the cortical, the medullar (pyramids) and the renal sinus (a fatty compartment located within the medial aspect of the kidney which contains the renal hilum)
References: Department of Radiology, Cluj County Emergency Hospital, Romania 2020
Step 4: Know the mimickers:
· Normal variants - Congenital Pseudotumors
· Acquired Pseudotumors - Infectious Masses, Vascular Structures, Some Benign Masses, Others entities
1. Congenital Pseudotumors:
- Hypertrophied Column of Bertin:

Fig. 4: Asymptomatic 45-year-old woman – Axial/Sagittal - view corticomedullary phase contrast enhanced CT shows a renal cortical tissue which separates the pyramids and enhance uniformly as renal cortex
References: Department of Radiology, Cluj County Emergency Hospital, Romania 2020
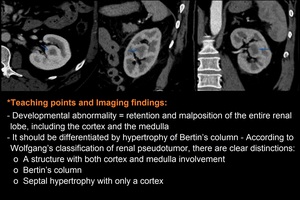
Fig. 5: Asymptomatic 45-year-old woman – Axial/ Sagittal/Coronal - view corticomedullary phase contrast enhanced CT shows a round mass adjacent to the outside of the renal pelvis and its density was enhanced to the same extent as the surrounding renal parenchyma
References: Department of Radiology, Cluj County Emergency Hospital, Romania 2020

Fig. 6: Asymptomatic 23-year-old woman – Coronal - view contrast enhanced CT nephrographic phase shows smaller, bilateral dysmorphic kidneys
References: Department of Radiology, Cluj County Emergency Hospital, Romania 2020

Fig. 7: Asymptomatic 67-year-old woman – Sagittal - view contrast enhanced CT shows lobulated renal cortices corresponding to an each renal pyramid; no hydronephrosis
References: Department of Radiology, Cluj County Emergency Hospital, Romania 2020

Fig. 8: Asymptomatic 45-year-old woman – Coronal-view contrast enhanced CT corticomedullary and nephrographic phase reveals a proeminent focal bulge on the lateral border of the left kidney
References: Department of Radiology, Cluj County Emergency Hospital, Romania 2020

Fig. 9: Asymptomatic 57-year-old man - The anomaly was suspected in a routine medical check-up; CT was done for confirmation and to rule out any urolithiasis: Axial/ Coronal/Reconstruction 3D view contrast enhanced CT corticomedullary phase shows inferior cross-fused right renal ectopia - both kidneys are fused on the right forming a unique enlarged kidney
References: Department of Radiology, Cluj County Emergency Hospital, Romania 2020

Fig. 10: Asymptomatic 38-year-old man - Axial/ Reconstruction 3D view contrast enhanced CT corticomedullary phase shows the kidneys are joined at their lower poles by a preaortic isthmus (arrow)
References: Department of Radiology, Cluj County Emergency Hospital, Romania 2020

Fig. 11: A: Asymptomatic 38-year-old man – Axial-view contrast enhanced CT corticomedullary phase shows incomplete rotation on the left kidney – renal pelvis (P) is located anteriorly; B: Asymptomatic 52-year-old woman – Sagittal/Coronal-view contrast enhanced CT corticomedullary phase reveals in the right kidney renal pelvis (P) and renal vessels are located superiorly
References: Department of Radiology, Cluj County Emergency Hospital, Romania 2020
2. Infectious Masses – Acute
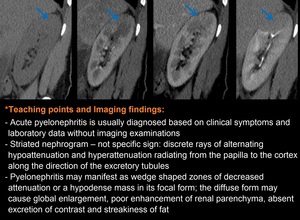
Fig. 12: Fig. 12. A 45-year-old woman with right flank pain, fever and hematuria for 3 days duration, not responding to medical - Sagittal-view non-contrast phase/ corticomedullary phase/nephrographic phase/pyelographic phase reveals a focal low attenuation region in the upper pole. Note the absence of a cortical rim sign
References: Department of Radiology, Cluj County Emergency Hospital, Romania 2020

Fig. 13: A 70-year-old woman with sepsis and diffuse abdominal pain with guarding - Axial-view non-contrast phase/ corticomedullary phase/nephrographic phase/pyelographic phase shows a well-defined cortical mass of low attenuation with a thick wall
References: Department of Radiology, Cluj County Emergency Hospital, Romania 2020

Fig. 14: A 69-year-old woman with left loin pain, known with spondilodyscitis T12-L1 - Axial and Coronal-view contrast enhanced CT non-contrast phase and nephrographic phase shows two thick walled perinephric fluid collections, one (blue arrows) in close contact with middle portion of left kidney and another one (red arrows) localized in the left psoas muscle. They were associated with abnormal thickening of the anterior and posterior perirenal fascia
References: Department of Radiology, Cluj County Emergency Hospital, Romania 2020

Fig. 15: A 45-year-old woman with dysuria and fever - 15 days. Coronal sections of delayed phase Contrast-enhanced computed tomography shows left duplex kidney with obstruction and hydronephrosis of lower moiety due to lower third ureteric calculus (blue arrows); walls of the pelvicalyceal system shows thickening and crescentic enhancement suggesting pyonephrosis; note patent superior ureter on pyelographic phase (red arrows)
References: Department of Radiology, Cluj County Emergency Hospital, Romania 2020
3. Infectious Masses – Chronic

Fig. 16: A 26-year-old man known with chronic pyelonephritis – Axial/ Sagittal/Coronal - view contrast enhanced CT nephrographic phase reveals multiple deep cortical scars on the both kidneys combining cortical retraction and deformation of the calyces and a small scarred kidney on the left
References: Department of Radiology, Cluj County Emergency Hospital, Romania 2020

Fig. 17: A 60-year-old diabetic female with urinary tract infection – Axial/Coronal-view non-contrast phase CT - globally enlargement of both kidneys (reniform enlargement), replaced by multiple rounded fluid-density areas. A staghorn calculus is present in the bilateral renal pelvis
References: Department of Radiology, Cluj County Emergency Hospital, Romania 2020
4. Infectious Masses – Parasitic Infection

Fig. 18: A 52-year-old man with an asymptomatic cystic mass in his right kidney detected by ultrasonography incidentally and diagnosed as renal hydatid cyst by further contrast-enhanced computed tomography scanning (well-defined complex cystic mass on the right kidney surrounded by thick walls) and surgery
References: Department of Radiology, Cluj County Emergency Hospital, Romania 2020
5. Vascular Structures

Fig. 19: A 73-year-old woman with abdominal pain - Axial-view non-contrast phase/Coronal-view/ Reconstruction 3D view contrast enhanced CT corticomedullary phase shows a bilobat focal dilatation of right renal artery
References: Department of Radiology, Cluj County Emergency Hospital, Romania 2020
6. Some Benign Masses

Fig. 20: Asymptomatic 57-year-old man - A mass was found in a routine abdominal ultrasound check-up; CT was done for its characterization: Axial – view non-contrast phase/corticomedullary phase/nephrographic phase reveals a partial exophytic round mass located in the right kidney with a uniform enhancement after contrast administration except a central scar that enhance slowly to the nephrographic phase
References: Department of Radiology, Cluj County Emergency Hospital, Romania 2020

Fig. 21: A 48-year-old woman presented for routine control - Axial-view contrast enhanced CT shows a well-defined, partially exophytic, lesion in the postero-medial cortex of the right in the lower pole region. This mass shows mildly hyperdense attenuation as compared to rest of the renal cortex, with some little areas of macroscopic fat (-9 HU); post contrast images reveals marked contrast enhancement within this lesion with attenuation values reaching up to level of 112 HU. The patient preferred to go to surgery and the diagnosis was confirmed
References: Department of Radiology, Cluj County Emergency Hospital, Romania 2020

Fig. 22: A 43-year-old man presented for routine control – MRI showed a T1 heterogeneous mass, well-defined, in the lower pole region of the left kidney; with some areas of Indian ink artifacts on opposed phase gradient-echo images (fatty components) and moderate reticular enhancement of the non-fatty components. 3D LAVA showing signal loss of the lesion due to fat saturation and contrast enhancement of the myovascular components
References: Department of Radiology, Cluj County Emergency Hospital, Romania 2020

Fig. 23: A 53-year-old man presented in the ED for sudden onset of pain in left flank, back and abdomen. On examination, she appeared in shock with cool extremities. Her abdomen was soft but tender generally with guarding in upper left quadrant. Axial-view unenhanced phase and contrast enhanced phase CT reveals a large left retroperitoneal hematoma from a left renal giant mass. The lesion has a large fatty component with abnormal vascularity, compatible with a large angiomyolipoma (Wunderlich syndrome). Note a small similar lesion (blue arrow)
References: Department of Radiology, Cluj County Emergency Hospital, Romania 2020
*Teaching points and Imaging findings:
- Renal angiomyolipoma (AML) is the most common type of benign solid renal tumor
- Renal AML can be classified according to amount of fat as fat rich, fat poor, or fat invisible
- Fat-invisible AML should be biopsied, and fat-poor AML requires further investigation to determine whether biopsy is necessary to differentiate it from renal cell carcinoma. If differentiation between AML and renal cell carcinoma is not clear with CT and MRI, percutaneous biopsy may be performed
- Enlarged renal AMLs can rupture; Wunderlich syndrome refers to spontaneous non-traumatic renal bleeding into the subcapsular and/or perirenal space
7. Others entities

Fig. 24: A 45-year-old woman with chronic kidney disease – Coronal-view non-contrast phase CT shows right renal hypoplasia with left compensatory hypertrophy
References: Department of Radiology, Cluj County Emergency Hospital, Romania 2020

Fig. 25: Asymptomatic 37-year-old man: Axial-view CT non-contrast phase/corticomedullary phase/nephrographic phase/pyelographic phase shows a well-defined hyperattenuating cortical renal lesion with no contrast enhancement
References: Department of Radiology, Cluj County Emergency Hospital, Romania 2020

Fig. 26: Asymptomatic 54-year-old woman: MR images shows a T1 and T2 hyperintense well-defined mass on the left kidney with no contrast enhancement
References: Department of Radiology, Cluj County Emergency Hospital, Romania 2020
*Teaching points and Imaging findings:
- Benign hyperattenuating renal cysts are classified as Bosniak II (diameter ≤ 3 cm) or Bosniak IIF (diameter >3 cm)
- On CT they appear as homogeneous, hyperdense cysts, with an attenuation of at least 70 HU and no contrast enhancement
- On MRI appear most commonly hyperintense on T1 and T2 weighted sequences. They may show fluid-iron levels because of dependent settling of methemoglobin containing sediments
- Common in polycystic renal disease, malignant cysts, trauma
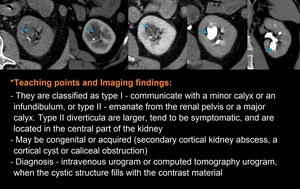
Fig. 27: Asymptomatic 50-year-old man: Axial - view non-contrast phase/corticomedullary phase/nephrographic phase/ pyelographic phase/ Coronal - pyelographic phase CT shows a endophitic renal cyst; the diagnosis is made in the pyelographic phase when the cystic structure fills with contrast material due to communication with the collecting system
References: Department of Radiology, Cluj County Emergency Hospital, Romania 2020
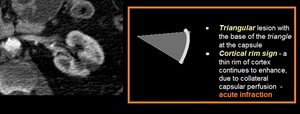
Fig. 28: A 52-year-old woman with abdominal pain – Axial - view contrast enhanced CT corticomedullary phase shows a hypointense triangular focal area in the middle portion of left kidney with a subtle capsule surface depression
References: Department of Radiology, Cluj County Emergency Hospital, Romania 2020
*Teaching points and Imaging findings:
- Imaging pattern: one or more focal, wedge-shaped or triangular areas of parenchymal defects that involve both the cortex and medulla and extend to the capsular surface
- Chronic infarcts are characterized by renal parenchymal interstitial fibrosis and capsule surface depression

Fig. 29: A 33-year-old man with renal failure – Coronal-view non-contrast phase CT reveals multiple small cysts in the both kidneys, some of them with hemorrhagic content
References: Department of Radiology, Cluj County Emergency Hospital, Romania 2020

Fig. 30: A 34-year-old man known with history of recent trauma - Axial-view contrast enhanced CT reveals two hypovascular cortical renal lesions (blue arrows), without laceration – grade 1 AAST(renal contusion). Note subcutaneous emphysema (yellow arrows)
References: Department of Radiology, Cluj County Emergency Hospital, Romania 2020

Fig. 31: A 59-year-old man - recent trauma - Axial-view contrast enhanced CT reveals laceration of the left kidney appearing as multiple opacification defects, without involvement of the collecting system; perirenal hematoma – grad 3 AAST
References: Department of Radiology, Cluj County Emergency Hospital, Romania 2020
*Teaching points and Imaging findings:
- The spectrum of renal injuries include: contusion, hematoma, laceration, hemorrhage, avulsion of the renal pedicle leading to devascularisation of the kidney pseudoaneurysm, AV fistula, renal artery thrombosis and transection or dissection
- The American Association for the Surgery of Trauma (AAST) renal injury scale is the most widely used grading system for renal trauma

Fig. 32: A 56-year-old man - recent trauma – Axial/Sagittal-view contrast enhanced CT reveals deep right perirenal hematoma
References: Department of Radiology, Cluj County Emergency Hospital, Romania 2020
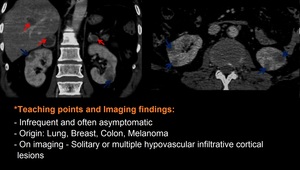
Fig. 33: A 67-year-old man known with Non-Small-Cell Lung Cancer – Coronal and axial-view contrast enhanced CT nephrographic phase reveals bilateral hypovascular and infiltrative cortical renal lesions (blue arrows). Note on coronal-view the bilateral suprarenal masses and a focal hypovascular lesion in the liver (red arrows)
References: Department of Radiology, Cluj County Emergency Hospital, Romania 2020

Fig. 34: A 54-year-old man with hematuria - Contrast enhanced CT scan demonstrates a mass within the left renal pelvis (arrows). The mass distends the renal pelvis (compare to the contralateral kidney) and shows relative high attenuation compared to the urine within the renal pelvis
References: Department of Radiology, Cluj County Emergency Hospital, Romania 2020

Fig. 35: A 75-year-old woman complaints of low back pain and loss of appetite – Axial-view CT corticomedullary phase reveals a solid hypovascular lesion at the pancreatic tail (red arrows), which had invaded into the middle anterior portion of left kidney
References: Department of Radiology, Cluj County Emergency Hospital, Romania 2020
Step 5: Focal renal mass –Some clues which helps us
- < 10 HU, no nodular enhancement or calcification → simple cyst
- 70 HU on unenhancement CT → hemorrhagic cyst
- 20 HU → previous images (first exam)
- Incidental cystic renal masses → Bosniak classification and management
- Incidental solid renal masses
→ Rule out non neoplastic etiology
→ Rule out fat → angiomyolipoma (no calcification)

Fig. 36: Proposed algorithm to avoid errors in detection in the evaluation of renal masses
References: Layra Ribeiro de Sousa Leão et all. (2019) Common pitfalls in renal mass evaluation: a practical guide. Radiol Bras. Jul/Ago;52(4):254–261

Fig. 37: Proposed algorithm to avoid errors in interpretation in the evaluation of renal masses
References: Layra Ribeiro de Sousa Leão et all. (2019) Common pitfalls in renal mass evaluation: a practical guide. Radiol Bras. Jul/Ago;52(4):254–261
Step 6: Aims of imaging – Our role as radiologists
- Detection
- Imaging features and differential diagnosis
- Avoid technical pitfalls of CT/MRI – they will not be considered in this paper
- Recommendations
*Many renal masses are either too small to be characterized
*Inability to use imaging alone to distinguish benign from malignant tumors
*In certain circumstances, percutaneous biopsy will be required to obviate unnecessary surgery
