Type:
Educational Exhibit
Keywords:
Performed at one institution, Not applicable, Retrospective, Image registration, Cancer, Surgery, Comparative studies, Biopsy, MR, CT, Paediatric, Head and neck, Eyes, Oncologic Imaging
Authors:
H. Souza, J. Albuquerque, R. Costa, V. Simonini, F. Miraldi, M. Decnop, M. F. Uberti; Rio de Janeiro/BR
DOI:
10.26044/ecr2020/C-13560
Background
Retinoblastoma (RB) is the most common malignant intraocular tumor in childhood, with an incidence of one for each 17.000 live births¹. It originates in the retina and belongs to a group of neoplasms with embryonic neuroblastic elements. Most cases are diagnosed within the first four years of life, with a median age at clinical presentation of 2 years for unilateral forms, and 1 year for bilateral form. RB is non-hereditary in two-third of cases, as a result of spontaneous RB-1 mutation in just one single retinal cell, and hereditary in one-third of cases, due to RB-1 mutation inherited from one parent or that occurs in an egg, sperm cell or just after fertilization. All bilateral forms, as well as 10–15% of unilateral forms, are related to the hereditary form of the disease.
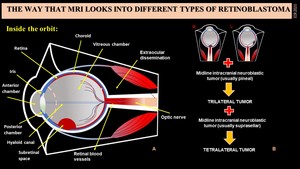
Fig. 1: A- Eye’s Anatomy and the relation to retinoblastoma. B- Trilateral and tetralateral scheme.
Patients usually present leukocoria (white pupil reflection) or strabismus. It may also be complicated and show additional findings like vitreous haemorrhage, retinal detachment, buphthalmos (due to angle-closure glaucoma), and proptosis. The diagnosis is usually established by fundoscopy and ultrasonography (US), both performed by the ophthalmologist. As an additional diagnostic tool, MRI plays a crucial role in determining the local extent and detecting associated brain abnormalities.
The MRI is the most accurate technique for diagnostic confirmation of RB, as well as to evaluate the extension of the disease and possible complications, therefore being used for pretreatment assessment. Computed tomography (CT) is nowadays avoided due to ionizing radiation and lack of additional diagnostic information. In contrast, US and MRI together are currently considered almost as accurate as CT for calcifications detection, which is present in approximately 95% of tumors, being a key finding to differentiate retinoblastoma from other mass lesions in a young child.
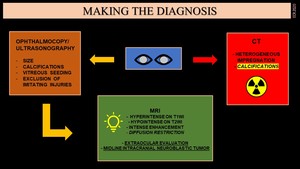
Fig. 2: How to make the diagnosis of retinoblastoma.


