ECR 2020 / C-13560
The Way that MRI Looks into Different Types of Retinoblastoma
Congress:
ECR 2020
Poster Number:
C-13560
Type:
Educational Exhibit
Keywords:
Performed at one institution, Not applicable, Retrospective, Image registration, Cancer, Surgery, Comparative studies, Biopsy, MR, CT, Paediatric, Head and neck, Eyes, Oncologic Imaging
Authors:
H. Souza, J. Albuquerque, R. Costa, V. Simonini, F. Miraldi, M. Decnop, M. F. Uberti; Rio de Janeiro/BR
DOI:
10.26044/ecr2020/C-13560
 hyperintense to vitreous humor on T1WI (A) and hypointense on T2WI (B), with restricted diffusion on DWI (C) and ADC-map (D). E) Large white mass on fundoscopy with proeminent feeder vessels (blue arrow) located at the macula causing reduced visual acuity.")
Fig. 3:
2 year-old girl with left retinoblastoma presenting with leukocoria. Axial MRI...
 and STIR hypointense (red arrows) mass occupying almost entirely the right globe and a retrolental retinal based mass in the left eye. The tumor volume is frequently inversely proportional to the size of the globe. C,D - 3 year-old girl with bilateral RB. Each of the eyeballs has a posterior endophitic lesion with some signal voids on STIR (blue arrows) corresponding to calcifications on CT (green arrows).")
Fig. 4:
A,B – 2 month-old baby with bilateral retinoblastoma presenting with...
 and low signal on STIR (blue arrows) compared to the vitreous. C,D - MRI T1WI FS + GD shows a vivid heterogeneous enhanced pineal (green arrows).")
Fig. 9:
11-month-old baby boy with trilateral retinoblastoma. A,B - MRI axial images...
 109:535–544.")
Fig. 10:
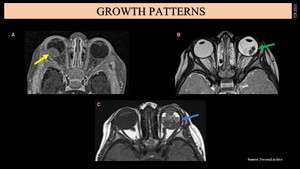
A – Axial MRI T1WI + Gd. B – Axial MRI T1WI + Gd.
 (yellow arrow). B- Subretinal T2 low sign mass (exophytic pattern) causing retinal detachment (green arrow). Note that there is an increase on anteroposterior eye diameter (buphthalmos). C- Both vitreous and subretinal (mixed growth pattern) T1 heterogeneous mass (blue arrow) associated with intraocular haemorrhage.")
Fig. 5:
A- Enhanced mass projecting into vitreous chamber (endophytic pattern) (yellow...
. B – 2-year-old boy with left RB. MRI axial images (T1 WI) show a bulky tumor filling almost the entire eyeball (green arrow). C – MRI axial T1 + GD images show a large relative hyperintense mass associated to haemorrhage in the right eye. The tumor has an extension to the crystalline lens (blue arrow).")
Fig. 6:
A –2-year-old girl with right retinoblastoma. MRI sagittal images show...
. B- 3-year-old boy with right RB. MRI axial T1 images show a bulky heterogeneous intraocular lesion and lateral retrobulbar mass (green arrow). C,D – 2-year-old girl with left RB. MRI axial T2 images show a retrolaminar and transcleral extension lesion (blue arrows) (C). Same patient months later (orange arrows) (D). Dramatic growth with skull base destruction (purple arrows) and anterior exophytic projection.")
Fig. 7:
A – 2-year-old girl with advanced left retinoblastoma with posterior...
 on MRI axial T2 (A) and sagittal T1 FS + GD images (B).")
Fig. 8:
4-year-old boy with retinoblastoma diagnosis presenting with multiple...
 without lesion enhacement on contrasted T1 images (green arrow). B– Persistent hyperplastic primary vitreous. 1-year-old boy also presenting with leukocoria. MRI axial T2 FS images show a slightly smaller left globe with a retrolental mass (purple arrow), hyperintense vitreous and a linear vessel along the hyaloid canal, also seen as an enhanced line on axial T1 FS + GD images (persistent Cloquet canal) (orange arrow). C- Coloboma. MRI axial T2/T1/ T1 FS + GD images show a focal discontinuity at the posterior eyeball wall (blue arrows). Embryologically, colobomas are due to failure of closure of the choroidal fissure.")
Fig. 11:
A– Coats disease. 3-year-old boy presenting with leukocoria and strabismus....