ECR 2020 / C-15364
The usefulness of ultrasound in the evaluation of central catheters in pediatrics. Where and how will it be?
Congress:
ECR 2020
Poster Number:
C-15364
Type:
Educational Exhibit
Keywords:
Not applicable, Image verification, Catheters, Ultrasound, Vascular, Paediatric, Management
Authors:
G. A. Averanga Ticona1, O. fernandez2, G. P. Larraín Balderrama1, E. Bejarano1, Y. P. Narváez Rojas1, J. Crosta1, L. Borrino1; 1Buenos Aires/AR, 2Pablo Nogues Buenos Aires/AR
DOI:
10.26044/ecr2020/C-15364

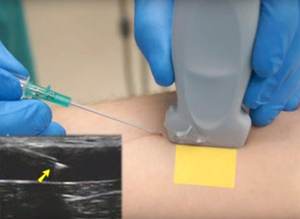
Fig. 1:
The ultrasound guide allows you to choose the best "target vessel", determine...

Fig. 2:
Indications for the placement of a central line.

Fig. 3:
Contraindications for the placement of a central line
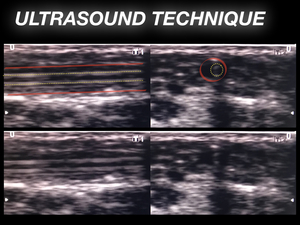
 or longitudinal ("in plane") position.")
Fig. 4:
The vessels can be located in transverse ("out of plane") or longitudinal ("in...
")
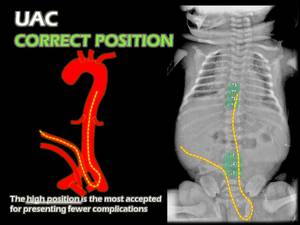
Fig. 5:
Graph of the correct location of Umbilical Arterial Catheters (UAC)
.")
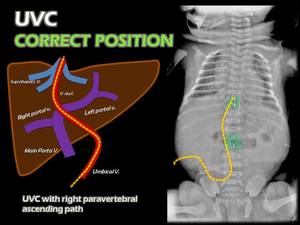
Fig. 6:
Graph of the correct location of Umbilical Venous Catheters (UVC).
.")
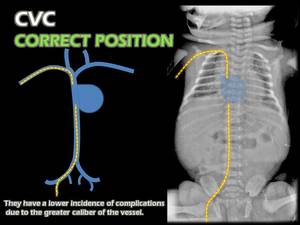
Fig. 7:
Graph of the correct location of Central Venous Catheters (CVC).

Fig. 8:
Wrong position. 2 months with subclavian catheter with abnormal positioning...

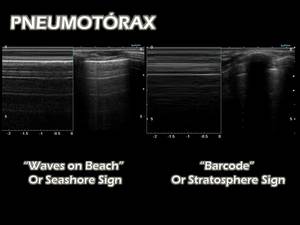
Fig. 9:
Pneumothorax by ultrasound. On suspicion of complication, ultrasound is useful...

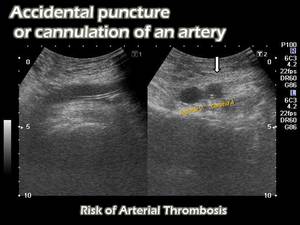
Fig. 10:
Accidental puncture or cannulation of an artery. It is usually found after a...

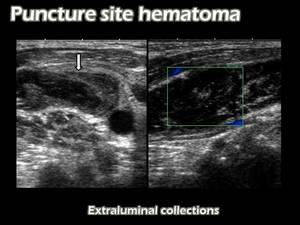
Fig. 11:
Juxta-jugular hematoma secondary to CVC placement.

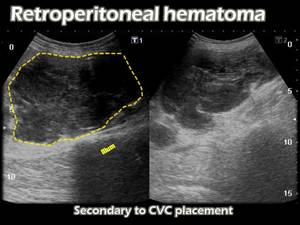
Fig. 12:
Retroperitoneal hematoma. Uncommon complication secondary to femoral...

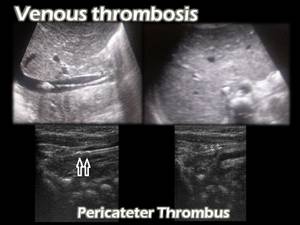
Fig. 13:
Venous thrombosis Pericateter thrombus is observed adjacent to the distal end...

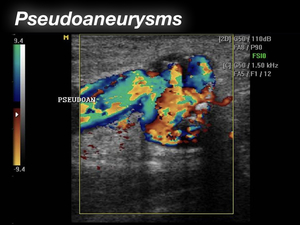
Fig. 14:
Pseudoaneurysm Secondary to vascular injury due to improper catheter placement....

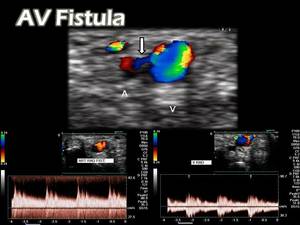
Fig. 15:
AV fistula The color Doppler examination shows turbulent arterial flows of low...

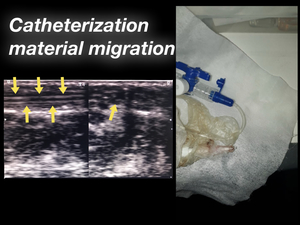
Fig. 16:
Catheterization material migration. 8 years, a catheter rupture occurs when...