ESSR 2017 / P-0303

Axial spondyloarthritis – the role of imaging in diagnosis and management
Congress:
ESSR 2017
Poster Number:
P-0303
Type:
Educational Poster
Keywords:
Musculoskeletal spine, Musculoskeletal joint, MR, CT, Conventional radiography, Staging, Complications, Arthritides
Authors:
A. P. Caetano, A. L. Proenca, S. Castro, M. F. Fontes; Lisbon/PT
DOI:
10.1594/essr2017/P-0303

Fig. 34:
Extensive bilateral bone-bridging with ankylosis of a significant portion of...

Fig. 35:
Near-complete ankylosis of both sacro-iliac joints with preservation of joint...
 and apparent bone-bridging of its posterior portion. Patient with AS.")
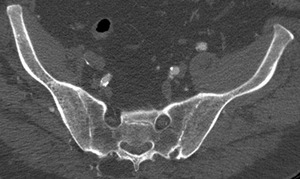
Fig. 30:
Right sacro-iliac joint space narrowing, joint space widening on the anterior...
; superior edge sclerosis with bone-bridging (capsule or ligamentous calcifications). Patient with AS.")
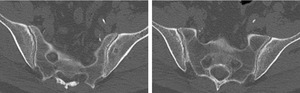
Fig. 31:
CT - coronal oblique reconstruction; bilateral joint space narrowing of the...

Fig. 37:
MRI - T1WI coronal oblique sections: bone bridging and ankylosis on several...
 of the ilium side of the sacro-iliac joints in patient with AS.")
Fig. 32:
Ferguson view - marked bone sclerosis (> 5 mm away from joint) of the ilium...

Fig. 33:
MRI - several sequences show: patchy bone changes with hypersignal on T1 and T2...
 are present near the iliac and sacral articular surface, more prominent at the inferior and anterior portion of the sacro-iliac joint. Patient with suspected AS.")
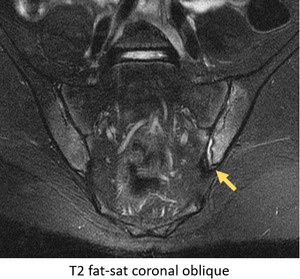
Fig. 22:
MRI - STIR coronal oblique sections: several small foci of bone marrow edema...
 on the sacral side of both sacro-iliac joints; there is also moderate synovial fluid on the left joint. Patient with Crohn's Disease.")
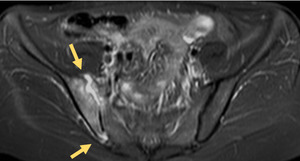
Fig. 23:
MRI - STIR coronal oblique sections: extensive bone marrow edema on the iliac...
. There is also extensive bilateral bone marrow edema. Patient with Crohn's Disease.")
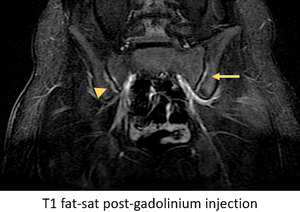
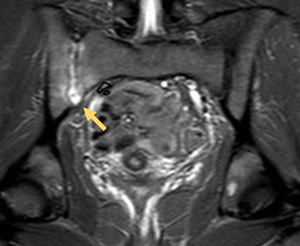
Fig. 21:
MRI - STIR coronal oblique slice: moderate synovial fluid on the left...
. On the right SI joint, there is contrast uptake by subchondral bone, indicative of osteitis (arrowhead).")
Fig. 25:
On the left SI joint, there are areas of contrast uptake at the synovial joint,...

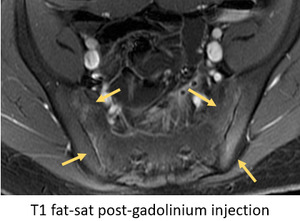
Fig. 24:
T1 fat-saturated images after gadolinium injection confirms that bone marrow...

Fig. 36:
CT coronal oblique reconstructions depict bilateral ankylosis of the SI joints...

Fig. 26:
T1 fat-saturated sequence after gadolinium injection shows extensive synovitis...

Fig. 27:
Marginal capsulitis on the superior and inferior edges of lfet SI joint.

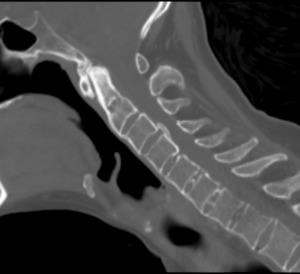
Fig. 58:
CT sagital slices - near-total ankylosis of the zygoapophyseal joints in...

Fig. 46:
Anterior and posterior syndesmophytes.

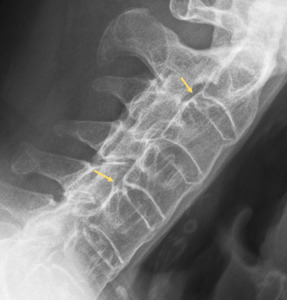
Fig. 59:
Radiograph - cervical oblique view - bone bridging of the inter-apophyseal...

Fig. 52:
Bridging syndesmophytes.

Fig. 56:
Dystrofic calcification of the intervertebral disks. "Shiny corners" due to...

Fig. 55:
"Shiny corners" on vertebral endplates with advanced syndesmophytes.

Fig. 57:
Dystrofic calcification of the intervertebral disks. "Shiny corners" due to...

Fig. 53:
Lateral syndesmophytes.

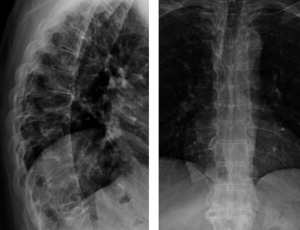
Fig. 62:
Marked osteopenia of the lumbar vertebrae in patient with advanced Ankylosing...

Fig. 47:
Railroad track sign in patient with Ankylosing Spondylitis.

Fig. 45:
Bone-bridging /ankylosis of cervical spine due to advanced syndesmophytes.

Fig. 50:
Posterior syndesmophytes.

Fig. 49:
Dorsal spine syndesmophytes.

Fig. 60:
Inter-spinous ligament calcification with Dagger Sign in patient with...

Fig. 48:
Lumbar spine syndesmophytes.
.")
Fig. 43:
Inter-apophyseal joint inflammation in patient with Ankylosing Spondylitis...
.")
Fig. 42:
Inter-apophyseal joint inflammation in patient with Ankylosing Spondylitis...
.")
Fig. 41:
Inter-apophyseal joint inflammation in patient with Ankylosing Spondylitis...

Fig. 61:
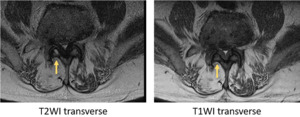
Fat-deposition on the subchondral plates of L4-L5, confirmed with...

Fig. 40:
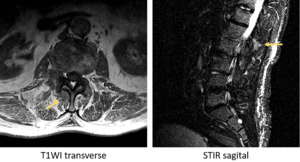
ASeptic spondylodiskitis - Andersson Lesion confirmed by excluding high-signal...

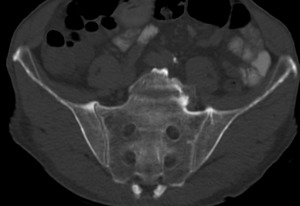
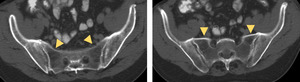
Fig. 38:
CT - coronal oblique reconstructions: juxta-articular osteoporosis in patient...

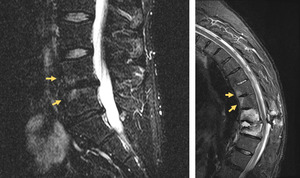
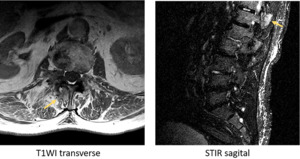
Fig. 39:
MRI - left - STIR sequence: bone marrow edema at the corners of the endplates...

Fig. 28:
Cortical bone erosions and pseudo-widening of the left SI joint.

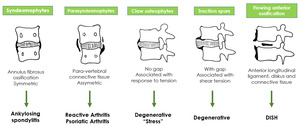
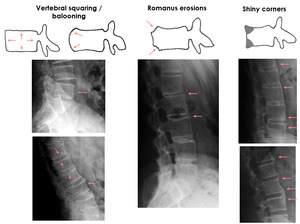
Fig. 44:
Patterns of para-vertebral ossification in different disorders.
; Romanus lesions with corner erosions (middle).")
Fig. 54:
Sclerotic bone changes of the vertebral endplates (left and right); Romanus...

Fig. 51:
Ligament calcification patterns.

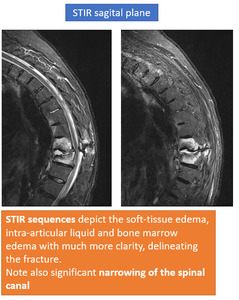
Fig. 65:
STIR sequences. Different sagittal planes are shown. Extensive intervertebral...

Fig. 66:
T1 fat-saturated sequence after gadolinium injection. Different sagittal planes...

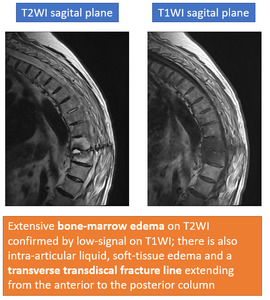
Fig. 63:
MRI sequences showing vertebral fracture.

Fig. 64:
MRI sequences showing vertebral fracture.