Retrospective review of 41 consecutive patients treated by US-guided corticosteroid injections at our institution.
Procedures performed from January 2014 to July 2017 were included.
Clinical outcomes (complete pain resolution,
partial pain resolution,
no significant pain relief and therapeutical failure-need for a new surgical procedure) were obtained from radiologist follow-up visits 6 and 12 weeks after the procedures,
and from medical records,
with a follow-up of 9 to 51 months.
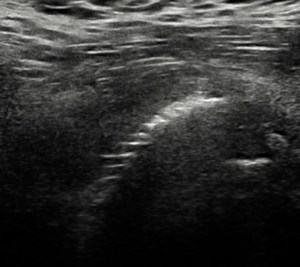
Fig. 1: Overhanging of the metallic surface of the prosthetic cup
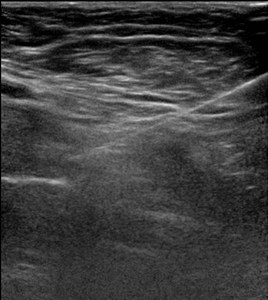
Fig. 2: Fine-needle corticosteroid inyection in the surface of the prosthetic cup
The CT findings obtained were: Overhanging acetabular cup,
fat infiltration and atrophy of psoas muscle,
other sources of pain detected on CT (heterotopic ossification,
screw malpositioning,
cement migration,
prosthetic shaft loosening,
pelvic bone Paget,
multiple myeloma lesions,
lumbar arthrodesis,
spondylolisthesis,
lumbar foraminal stenosis.
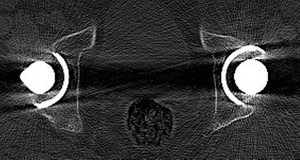
Fig. 3: Left THR retroversion with extensive overhanging of the acetabular cup

Fig. 4: Fat infiltration and atrophy of psoas muscle
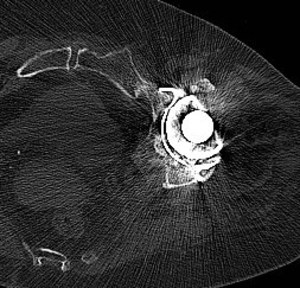
Fig. 5: Cement migration
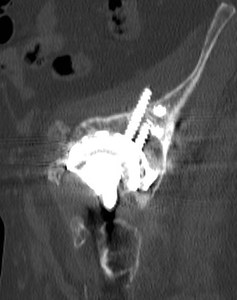
Fig. 6: Screw malpositioning into iliac muscle
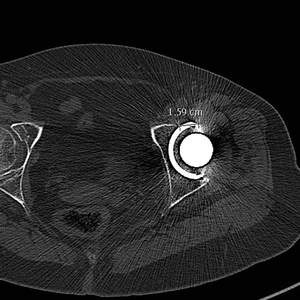
Fig. 7: Axial measure of the overhanging acetabular cup
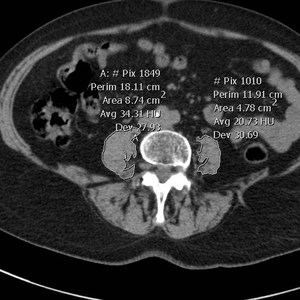
Fig. 8: Measuring of density and cross sectional area of the psoas muscles at L4 vertebral body
Atrophy of psoas muscle: Measuring the area of both psoas muscles at L4 (Kamaz et al),
we consideres differences with healthy side of <10% as no atrophy; 10-40% as grade 1 atrophy; >40% as grade 2 atrohpy
Fat infiltration: Rated as fat infiltration when density of the area is <30 UH (Cleary et al)
