ESSR 2018 / P-0012
Clinic outcome of US-guided injection of corticosteroids for iliopsoas impingement after total hip replacement
Congress:
ESSR 2018
Poster Number:
P-0012
Type:
Scientific Poster
Keywords:
Interventional non-vascular, Musculoskeletal joint, Extremities, Percutaneous, Ultrasound, CT, Puncture, Treatment effects, Prostheses, Outcomes, Inflammation
Authors:
D. Quintana Blanco1, G. Larrañaga Hernando2, A. Ostapenko1, N. Serrano Usaola1, S. Beltran de Otalora Garcia2, M. Martín Egaña1; 1Vitoria/ES, 2Vitoria-Gasteiz/ES
DOI:
10.1594/essr2018/P-0012

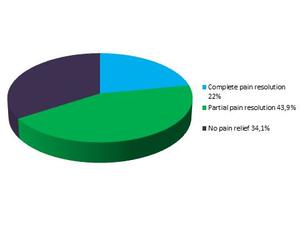
Fig. 9:
General clinical improvement results

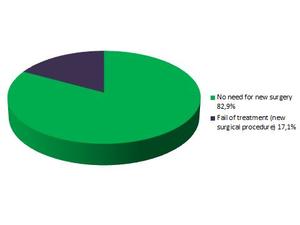
Fig. 10:
Failure of treatment, considered as the need for new surgical treatment

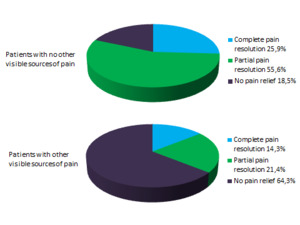
Fig. 11:
Differences in outcome depending on other visible causes of pain in CT

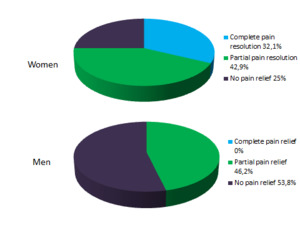
Fig. 12:
Outcome depending on gender

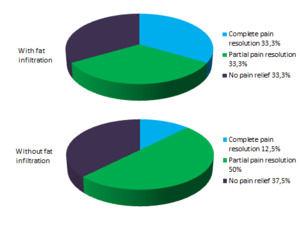
Fig. 13:
Results depending on fat infiltration

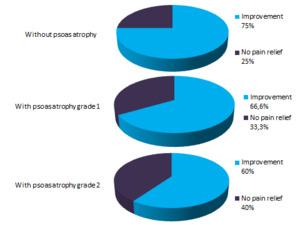
Fig. 14:
Results depending on psoas atrophy