Anatomy
Anatomically each meniscus is divided into 3 (thirds) longitudinal segments:
1) the anterior horn
2) body(middle third)
3) posterior horn
Each meniscus measures between 4–7 mm in height,
tapering to a thin,
sharp inner margin.
Due to their fibrocartilaginous content both the medial and lateral menisci classically demonstrate diffuse low SI on all MRI imaging sequences.
On the peripheral slice sagittal images the menisci demonstrate the classical bow-tie appearance which represents the body Fig. 2 .
The anterior and posterior horns are typically demonstrated as triangular structures with sharply pointed inner margins.
On the coronal views of the meniscus the anterior and posterior horns appear as band like structures with the body of the meniscus depicted as a triangle
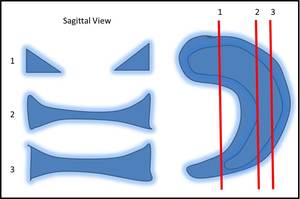
Fig. 2: Schematic diagram showing the various appearances of the meniscus in relation to the sagittal MRI plane. Note how the shape changes from the typical bow tie appearance to the separated triangle as you traverse from the outer to the inner edge.
The lateral genicular arteries (medial and lateral divisions) supply the menisci in three well described vascular zones Fig. 3 .
1) Peripheral very vascular RED-RED zone (<3mm from the capsule)
2) Middle low vascular RED-WHITE zone (3-5mm from the capsule)
3) Inner non vascular WHITE-WHITE zone (5mm from the capsule)
The relevance of the above is that a peripheral tear is more likely to heal with just conservative treatment alone due to its increased vascular supply.
It is important to note that if arthroscopy was considered in these type of tears,
the defect may not be seen as they would have most likely healed.
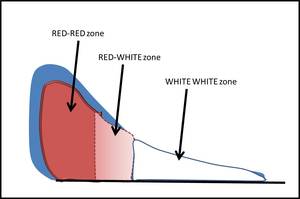
Fig. 3: Schematic diagram showing the various described vascular zones of the meniscus as it would appear on a coronal MRI. It is important to note that the periphery is the most vascular part, hence subtle areas of increased signal can represent vessels rather than tears or degeneration.
The Medial Meniscus (MM)
The MM is less mobile compared to the lateral meniscus as it is more tightly adhered to the joint capsule.
As a result of this attachment it is more likely to account for the increased incidence of MM injury/tears.
The anterior horn of the MM is described as having two segments and is roughly a 1/3rd smaller in size to the posterior horn of the MM.
The first segment is the anterior-inferior section where there is attachment of the MM to the medial tibial spine.
The second segment is the posterior-superior segment which gives rise to the transverse intermeniscal ligament ( Fig. 4 ).
The posterior horn of the MM attaches via the meniscal root to the tibial insertion of the PCL.
The function of this attachment is to prevent the meniscus from extruding.
The periphery of the MM is attached to the femoral condyle and tibial plateau by the deep portions of the MCL (the menisco femoral and meniscotibial ligaments) Fig. 5 .
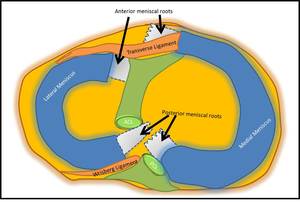
Fig. 4: Schematic diagram demonstrating the approximate positions of the anterior and posterior meniscal roots. Note the two segments of the anterior horn of the medial meniscus; The first segment is the anterior-inferior section where there is attachment of the MM to the medial tibial spine. The second segment is the posterior-superior segment which gives rise to the transverse intermeniscal ligament
There is attachment of the peripheral MM to the femoral condyle and tibial plateau by the deep portions of the MCL (the menisco femoral and meniscotibial ligaments) Fig. 5.
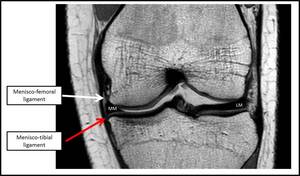
Fig. 5: Coronal T1W image of the right knee demonstrating the menisco-femoral ligament (WHITE ARROW) and menisco-tibial ligament (RED arrow) of the medial meniscus (MM). LM-Lateral meniscus.
References: Department of Radiology, Queen Elizabeth Hospital Birmingham
At the innermost section of the posterior horn there is a variable amount of fibrofatty connective tissue and occasionally a small recess can be present at the menisco-capsular junction.
Note that this recess does not extend all the way inferiorly or superiorly which would otherwise suggest a MM tear.
The transverse anterior intermeniscal ligament (geniculate ligament) runs between the anterior medial and lateral menisci.
It is said to be present in up to 83% of knees on MRI with its function mainly for stabilisation of the anterior horn of the MM. Its can get trapped/injured during a tibial eminence fracture and should be looked for when suspecting these injuries.
On MRI a low SI fibrous band through the posterior portion of Hoffas fat pad is seen.
The Lateral Meniscus (LM)
The LM has equally sized anterior and posterior horns and is notably smaller than the MM.
The tibial attachment of the anterior horn is anterior to the tibial spine but posterolateral to the tibial attachment of the ACL. The tibial attachment of the posterior horn is posterior to the tibial spine and importantly anterior to the posterior horn of the MM attachment ( Fig. 4 ).
Note that the LM at the postero-lateral corner has a loose attachment to the joint capsule.
The popliteo-meniscal fascicles provide a direct attachment of the LM to the popliteus tendon (best appreciated on sagittal T2 sequences).
The popliteo-meniscal fascicles prevent excessive forward movement of the lateral meniscus during extension of the knee.
The Meniscofemoral Ligaments
There are two lateral meniscus meniscofemoral ligaments Fig. 6 :
1) Anterior to the PCL runs the ligament of Humprey
2) Posterior to the PCL runs the ligament of Wrisberg
They attach the posterior horn of the lateral meniscus to the PCL or medial margin of the medial femoral condyle. Functionally they are there to stabilise the posterior horn of LM.
One of these ligaments are usually identifiable in patients on MRI.
The thickness of the ligament of Humphrey can vary and occasionally can be mistaken for a bucket handle tear ‘double PCL’ sign.
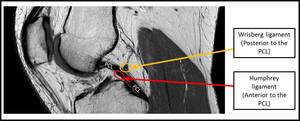
Fig. 6: Sagittal PDW MRI image showing the two main posterior meniscofemoral ligaments related to the PCL. The Wrisberg ligament (posterior meniscofemoral ligament) and the Ligament of Humphrey (anterior meniscofemoral ligament).
References: Department of Radiology, Queen Elizabeth Hospital Birmingham
Anatomical Variants – The Discoid Meniscus
This is a congenital anomaly where either the MM or LM has a thickened disc shape ( Fig. 7 ).
It is usually more common on the LM and defined in a meniscus having a width of >15mm.
A Wattanbe classification system for discoid meniscus exists and is as follows:
- Type I – Incomplete – Partial coverage of the tibial condyle
- Type II –Complete- Whole of tibial condyle covered
(the above two are defined based to the degree of tibial plateau coverage)
- Type II – Wrisberg (Rare type with nearly normal morphology but lacking posterior capsular attachments) As a result this type is associated with snapping knee syndrome in children and in rare occurences the posterior horn can flip anteriorly mimicking a bucket handle tear.
On MRI a discoid meniscus can be identified when there is meniscal continuity on at least 3 or more 5mm sagittal slices.
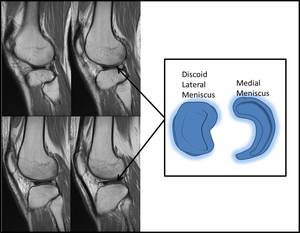
Fig. 7: Sagittal PD sequences of the right knee lateral meniscus. The sequential slices demonstrate a discoid meniscus with continuity across at least 4 sequential images. The schematic diagram on the right demonstrates the loss of the normal c shape of the lateral meniscus in keeping with a discoid meniscus.
References: Department of Radiology, Queen Elizabeth Hospital Birmingham
Meniscal Tears
MRI findings: On MRI imaging there are both primary findings and secondary features to suggest a meniscal tear.
Primary findings of meniscal tear are as follows:
A) Increased intramensical signal that reaches an articular surface on more than one image is classical for a meniscal tear.
The ‘two-slice touch’ rule is a well-known term and is defined by the high SI breaching the articular surface on two images (either on the same or different planes).
It has been shown that if only one slice demonstrates the high SI articular breach,
55% of these case will have a positive tear on arthroscopy.
It is therefore pertinent that as radiologists we correlate high SI meniscal-articular breaches with extra care and look on different planes at the same location.
B) A blunting or small meniscus demonstrated an abnormal meniscal morphology and suggests meniscal tissue loss.
This should prompt a search for a displaced fragment.
Secondary features of meniscal tear have several varieties and are as follows:
A) The presence of a parameniscal cyst has a strong association with an underlying meniscal tear ( Fig. 8 ).
B) Bone marrow oedema in the tibia especially underneath a meniscus can indirectly indicate an underlying tear
C) Disruption of the posterosuperior popliteo-meniscal fascicle is strongly associated with a LM posterior horn tear
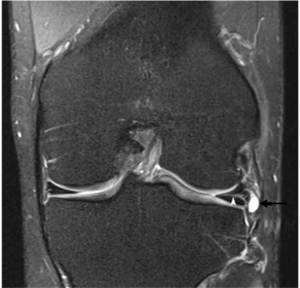
Fig. 8: Coronal PD FS MRI image demonstrating a hyperintense parameniscal cyst (black arrow) arising from a known horizontal meniscal tear (white arrowhead) . On subsequent sequences one can see direct communication between the two.
References: Department of Radiology, Queen Elizabeth Hospital Birmingham
Classification of meniscal tears
The generally accepted classification of meniscal tears are classified as follows:
- Radial tears
- Longitudinal tears
- Horizontal tears (usually degenerative tears)
- Flap tears
- Complex tears
Radial tears
This is a vertical tear which arises from the free edge of the meniscus and runs perpendicular to the long axis of the meniscus.
They can be small or large.
Smaller radial tears are only limited to the free edge of the meniscus and are associated with meniscal extrusion.
Larger radial tears involve and run through the whole width of the meniscus and should be described as partial or complete.
The latter is associated with developing premature degenerative changes and severely compromising meniscal function.
Important locations to look for radial tears are the posterior horns of both menisci and the body of the LM.
Imaging findings of radial tears:
Radial tears are commonly diagnosed via one of the following four signs:
1) Vertical high SI passing through the meniscus on one slice – CLEFT sign Fig. 9
2) Vertical high SI passing though the meniscus on consecutive sagittal slices – MARCHING CLEFT SIGN
3) At the inner free edge there is sudden termination of the normal triangular meniscal contour – TRUNCATED TRIANGLE SIGN
4) High SI meniscal fragment as the image slice is directly in line with the tear – GHOST MENISCUS SIGN
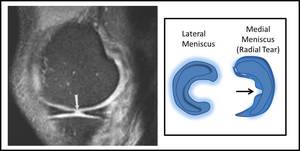
Fig. 9: (Left MRI image) demonstrating truncation of the free edge of the medial meniscus (WHITE ARROW). Schematic diagram (right) demonstrating the tear in the free edge of the medial meniscus. Findings are consistent with a radial tear.
References: Department of Radiology, Queen Elizabeth Hospital Birmingham
Longitudinal Tear
These tears run parallel (at a constant distance to the peripheral margin) to the long axis of the meniscus.
Either one or both of the superior or inferior articular margin can be breached and are strongly associated with ACL injury/rupture.
Bucket handle tears (more common in the MM) are described when a tear extends through the whole length of the meniscus causing the inner fragment to be flipped into the intercondylar notch.
Patients with a bucket handle tears typically present with locking.
Imaging findings of longitudinal tears
A vertically orientated linear increased SI focus within the meniscus (usually in the outer third of the meniscus) which either breaches the inferior or superior articular surface or both.
A bucket handle tear has specific imaging signs:
- Double PCL sign – where the meniscal fragment is noted parallel and anterior to the PCL and noted on both the coronal and sagittal images ( Fig. 10 ).

Fig. 10: Sagittal image showing a classic double PCL sign in a bucket handle tear of the medial meniscus and schematic diagrammatic representation of the types of longitudinal tear that can occur.
References: Department of Radiology, Queen Elizabeth Hospital Birmingham
- Intercondylar notch fragment sign – a displaced flipped fragment is noted within the intercondylar notch and adjacent to the tibial spine
- Flipped meniscus sign – here the displaced posterior horn lies anterior and adjacent to the anterior horn making the anterior horn exceptionally large on imaging Fig. 11
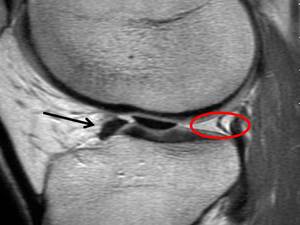
Fig. 11: Image showing the flipped meniscus sign the posterior horn lies anterior to the anterior horn of the medial meniscus (BLACK ARROW). Occasionally it is difficult to identify the two fragments as separate structures. Note an empty posterior horn (RED CIRCLE).
References: Department of Radiology, Queen Elizabeth Hospital Birmingham
- Absent bow tie sign – This more specifically referred to the residual meniscus where the body of the torn meniscus is noted on only 1 sagittal image or is completely absent ( Fig. 12 )
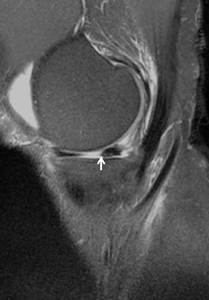
Fig. 12: Image showing the absent characteristic bow tie configuration of the meniscus (WHITE ARROW). Findings are consistent with a bucket handle tear.
References: Department of Radiology, Queen Elizabeth Hospital Birmingham
Less frequently:
- Double ACL sign – where the LM displaced tear fragment lies posteriorly and inferiorly to the ACL
- Truncated meniscus sign – on coronal imaging,
the inner margin of the meniscus appears blunted
- Quadruple cruciate sign – on the rare occurrence where there are both LM and MM bucket handle tears resulting in 4 structures within the intercondylar notch (both flipped menisci and the two cruciates).
Horizontal tears
These tears are cleavage type tears where extension of tear occurs in a parallel plane to the tibial plateau and involving either one of the articular surfaces or free edge.
They are often noted in the posterior horns but can also propagate into the body or anterior horn.
This results in the meniscus being divided into both superior and inferior sections.
Typically these are secondary to a degenerative cause and often noted in patients >40 years.
This tear is often associated with a parameniscal cyst.
Imaging findings of Horizontal tears:
A high SI line which is horizontally running though the meniscus (with or without) extension of tear towards the tibial articular surface Fig. 13
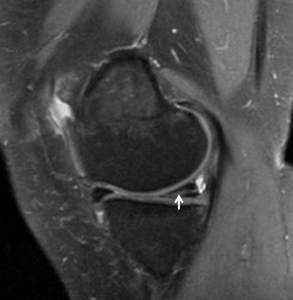
Fig. 13: Image showing a fluid intensity signal traversing horizontally through the meniscus(WHITE ARROW). This breeches the inferior tibial articular surface and is consistent with a horizontal longitudinal tear. Note the adjacent parameniscal cyst.
References: Department of Radiology, Queen Elizabeth Hospital Birmingham
Flap tears
When a torn meniscus becomes displaced or can be displaced during arthroscopy.
Similar to any displaced fragment,
symptoms include pain and locking.
Flap tears can be classified based on the tear type predominance – typically vertical and horizontal flap tears.
- The horizontal flap tear commonly affects the MM.
It is good practice to look posteriorly near the intercondylar notch or posterior to the PCL as most fragments displace here. A specific and uncommon type of horizontal flap tear is the hemi-bucket handle tear where within the MM there is an inferior articular horizontal flap tear.
This results in the meniscal tissue to displace towards the intercondylar notch.
This should be distinguished from a bucket handle tear as the former has a poor outcome for the patient if left untreated and can influence surgical management.
- Vertical flap tears are described as ‘parrot beak’ tears ( Fig. 14 ).
They usually start as a radial tear and then develop a longitudinal tear component resulting is a small section of free floating unstable meniscal tissue.
If this tissue is displaced it usually stays central in location.
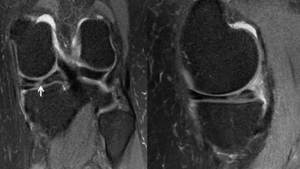
Fig. 14: Image showing a typical pattern of a parrot beak tear: Note the initial radial tear at the inner free edge of the medial meniscus(WHITE ARROW). There is further high signal extending out in a longitudinal fashion. If this progresses further the tear can detach and become unstable.
References: Department of Radiology, Queen Elizabeth Hospital Birmingham
Special types of meniscal injury
- Meniscal Root injury
- Ramp lesion
- Meniscal cysts
- Meniscal subluxation
- Meniscocapsular separation
- Meniscal degeneration
Meniscal root injury
LM root tears are usually related to trauma and are frequently associated with ACL injury/rupture in comparison to posterior horn MM root tears,
which mainly occurs secondary to degenerative meniscal pathology.
Imaging findings of meniscal root tear: The presence of high SI within a MM root which does not reach the articular surface is a specific sign that can represent a poorly functioning root attachment and likely represents a partial incomplete tear.
This can be an early predictive sign of subsequent root tearing and shout be appropriately reported to the clinician. Complete tears on MRI are demonstrated as a total discontinuity of the meniscal root and best appreciated on coronal images showing a vertical linear high SI defect and a ghost sign on sagittal sequences ( Fig. 15 ).
Meniscal extrusion is noted in those that have posterior horn MM tears.
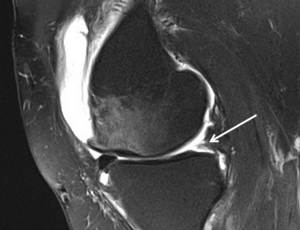
Fig. 15: Image showing increase signal at the posterior horn (WHITE ARROW) which is oedematous and less visible when compared to the anterior horn, so called 'ghost sign.'
References: Department of Radiology, Queen Elizabeth Hospital Birmingham
Medial meniscal ramp lesion
This is related to disruption of the peripheral meniscocapsular attachments of the MM posterior horn.
(Figure 16).
On imaging the most specific sign is the visualisation of a thin high SI in between the posterior horn of the MM and the postero-medial capsule.
This is commonly seen in ACL injuries and confers an additional element of instability Fig. 16 .

Fig. 16: Image showing increased irregular signal at the most peripheral aspect of the posterior medial meniscus. This tends to be only seen on the most peripheral 1-2 slices and is termed RAMP lesion. It is commonly seen as an associated sign of instability among the ACL spectrum of injuries.
References: Department of Radiology, Queen Elizabeth Hospital Birmingham
Meniscal subluxation
This is when meniscal extrusion/protrusion occurs.
This is roughly defined when there is >3mm of MM and >1mm of LM edge of the meniscus noted to be beyond the margin of the tibial plateau.
Apart from being associated with meniscal tear (particularly radial tears or meniscal root tears),
meniscal extrusions can also be noted in ACL injury,
joint effusion,
OA and severe meniscal degeneration.
Parameniscal/intrameniscal cysts:
Meniscal cysts are thought to arise as joint fluid passes through a meniscal tear from the joint.
They are often seen in men <40 yrs and are often asymptomatic. These cysts can be classified as an parameniscal cyst,
adjacent to the meniscus in associated with a tear or infrenquently intrameniscal,
within the meniscus ( Fig. 17 ).
Imaging findings: On MRI the typical presentation is a well defined fluid SI lesion with contact to a meniscal tear.
If it is adjacent to the meniscus then it is parameniscal.
If it is within the meniscus then it is intrameniscal.
Internal septation can be normal findings.

Fig. 17: Image showing complete replacement of the normal substance of the posterior horn of the medial meniscus with fluid signal, consistent with an intra meniscal cyst
References: Image taken from: https://www.orthobullets.com/knee-and-sports/3006/meniscal-cysts
Meniscocapsular separation
This often occurs on the MM where the meniscus is noted to separate from the capsule.
The meniscofemoral and meniscotibial ligaments (deep MCL) are torn.
A degree of meniscal instability is often noted.
The tear involves the RED zone and therefore healing occurs frequently.
On the LM,
in the post traumatic context a ‘floating meniscus’ sign may be noted.
This is where the meniscus is surrounded by fluid suggesting a tear of the popliteomeniscal fascicles and meniscal avulsion from the tibia.
Imaging findings: MRI will demonstrated meniscal displacement and fluid in between the meniscus and the capsule Fig. 18 .
Irregular high SI at the meniscofemoral and meniscotibial ligaments suggest a meniscal corner tear
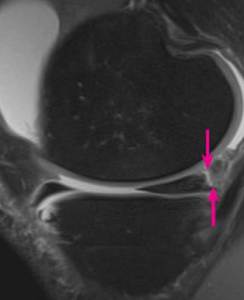
Fig. 18: Image: Sagittal proton density weighted MRI shows a rim of fluid intensity signal between the posterior horn of the medial meniscus and capsule indicating menisco-capsular separation.
References: Taken from: https://www.msdmanuals.com/professional/professional/multimedia/v13948093
Meniscal Degeneration
This is a commonly seen phenomenon which occurs in the meniscus with advancing age.
Although small interstitial tears can develop in severe degeneration they have no clinical relevance and do not represent a risk factor for a meniscal tear.
In the elderly degenerative knee,
fraying and irregular contouring of the menisci are seen.
MRI will demonstrate an increased SI on fluid sensitive sequences which importantly do not specifically reach the articular surface.
A grading system for the intrameniscal signal intensity is as follows Fig. 19 :
Grade 1 – Small focus of intrameniscal signal not reaching the articular margin
Grade 2a – Linear focus of intrameniscal signal not reaching the articular margin
Grade 2b – Abnormal intrameniscal signal reaching the articular margin on a single image
Grade 2c – Wedge shaped intrameniscal signal with no extension into the articular margin
Grade 3 – Complex intrameniscal signal reaching the articular surface – meniscal tear
Grade 4 – Meniscal fragmentation
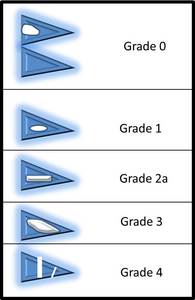
Fig. 19: Schematic diagram of the classification of meniscal tears. Note that Grade 2 tears can be sub divided onto a,b and c (not shown) with increasing severity of intra meniscal signal.
Meniscal tear management
There are both conservative and surgical options and heavily based on the imaging findings.
Preservation of as much meniscal tissue is crucial as the amount of meniscal tissue resected is heavily correlated with the severity of OA. Tears that are peripheral or more stable (within 3mm of the meniscocapsular junction) have a high chance of healing and therefore managed more conservatively.
Surgical management is based on the type of tear and can vary from simple meniscal repair to partial/complete meniscectomy.




 and menisco-tibial ligament (RED arrow) of the medial meniscus (MM). LM-Lateral meniscus. References: Department of Radiology, Queen Elizabeth Hospital Birmingham")
 and the Ligament of Humphrey (anterior meniscofemoral ligament). References: Department of Radiology, Queen Elizabeth Hospital Birmingham")

 arising from a known horizontal meniscal tear (white arrowhead) . On subsequent sequences one can see direct communication between the two. References: Department of Radiology, Queen Elizabeth Hospital Birmingham")
 demonstrating truncation of the free edge of the medial meniscus (WHITE ARROW). Schematic diagram (right) demonstrating the tear in the free edge of the medial meniscus. Findings are consistent with a radial tear. References: Department of Radiology, Queen Elizabeth Hospital Birmingham")

. Occasionally it is difficult to identify the two fragments as separate structures. Note an empty posterior horn (RED CIRCLE). References: Department of Radiology, Queen Elizabeth Hospital Birmingham")
. Findings are consistent with a bucket handle tear. References: Department of Radiology, Queen Elizabeth Hospital Birmingham")
. This breeches the inferior tibial articular surface and is consistent with a horizontal longitudinal tear. Note the adjacent parameniscal cyst. References: Department of Radiology, Queen Elizabeth Hospital Birmingham")
. There is further high signal extending out in a longitudinal fashion. If this progresses further the tear can detach and become unstable. References: Department of Radiology, Queen Elizabeth Hospital Birmingham")
 which is oedematous and less visible when compared to the anterior horn, so called 'ghost sign.' References: Department of Radiology, Queen Elizabeth Hospital Birmingham")



 with increasing severity of intra meniscal signal.")