Horner’s syndrome occurs when there is disruption to the oculosympathetic pathway.
The pathway takes a circuitous route from its central origin to its distal innervation of the orbit.
Subsequently,
the pathway can be interrupted at a number of different points along its route,
and by a variety of diseases (1).
The clinical description of oculosympathetic paresis was first described as long ago as 1727 where it was first noted as a complication during experimental intercostal nerve transections in dogs.
The syndrome takes its name from Swiss ophthalmologist Johann Freidrich Horner,
one of the first physicians to recognise the link between eye disease and systemic diseases of the body in 1869 (2).
Disruption of the oculosympathetic pathway at any point along it’s length results in ptosis.
This is a consequence of absent sympathetic innervation to the superior tarsal muscle (Müller’s muscle).
Slight lower lid elevation and narrowing of the palpebral fissure also occur.
Loss of sympathetic innervation to the pupillary muscles results in an imbalance between pupillary dilators (sympathetic) and pupillary constrictors (parasympathetic).
This imbalance manifests as pupillary miosis and anisocoria as parasympathetic supply exceeds the effect of sympathetic fibres ( Fig. 1 ).
Hemifacial anhidrosis (loss of sweating on the affected side of the face) occurs if the lesion disrupting the oculosympathetic pathway is proximal to the superior cervical ganglion.
This results from disruption to fibres supplying sweat glands of the face (3).
Enophthalmos (sunken globe) is also an associated clinical feature.
Figure 1 Sympathetic Fibres Entering the Orbit
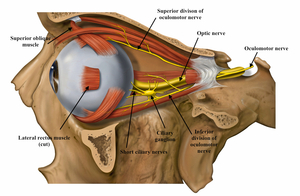
Fig. 1: The optic nerve can be seen entering the posterior aspect of the globe. The ciliary ganglion and branches of the oculomotor nerve carrying sympathetic fibres are visualised; these fibres innervate the superior tarsal muscle and lower lid small muscles as well as the pupillary dilators.
References: Patrick J. Lynch, medical illustrator; C. Carl Jaffe, MD, cardiologist. Reproduced with permission. Anatomical labels inserted by Lucy Childs with permission.
Anatomy of the Oculosympathetic Tract: A three neuron arc
First order neurons
Sympathetic innervation of the eye is based on a three neuron arc.
The ‘first-order’ central fibres of the pathway originate in the posterolateral aspect of the hypothalamus.
These pre-ganglionic fibres descend caudally through the tegmentum of the midbrain and pons.
Fibres then course anteriorly at the pontomedullary junction to lie anterior to the inferior olivary nucleus in the medulla.
Relevant adjacent structures include the spinothalamic tract (sensory pathway involved in pain,
temperature,
and coarse touch) and vestibular structures (balance).
From here the fibres descend into the cervical cord to terminate in the intermediolateral cell column of the spinal cord at C8-T2,
also known as the ciliospinal centre of Budge ( Fig. 2 ).
Figure 2 The Oculosympathetic Pathway
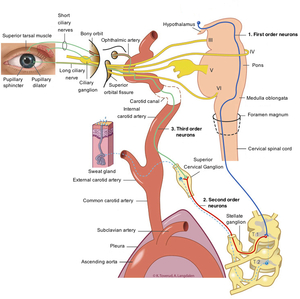
Fig. 2: The Oculosympathetic Pathway
References: Reproduced with permission from Anne Langdalen and Kari C. Toverud MS CMI. Image originally published with Norwegian labelling at: Ervervet Horners syndrom, Tidsskr Nor Legeforen 2011; 131: 950-4
Second order neurons
The second order pre-ganglionic neurons take a more circuitous course through the upper chest and neck.
Most of these fibres leave the spinal cord at the T1 level with the first ventral thoracic root (some fibres also leave via C8 and T2 ventral roots).
The neurons join the paravertebral cervical sympathetic chain and ascend in close relation to the lung apex,
an important site of pathology.
Fibres traverse the inferior cervical ganglion heading cranially towards the middle cervical ganglion ( Fig. 3 ).
Figure 3 The cervical ganglia
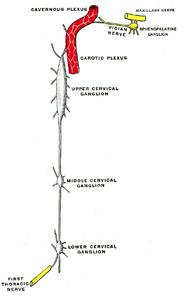
Fig. 3: The Cervical Sympathetic Ganglia
References: 20th U.S. edition of Gray's Anatomy of the Human Body. Originally published in 1918. Reproduced with permission.
The inferior cervical ganglion lies between the transverse process of C7 and neck of the first rib.
This ganglion may be fused with the first thoracic ganglion to form the ‘stellate ganglion.’ The vertebral artery lies anterior to the stellate ganglion; the pleural surface of the lung lies inferiorly.
As oculosympathetic fibres ascend towards the middle cervical ganglion they divide into two tracts.
One tract passes anterior to the subclavian artery,
the other passes posteriorly creating a loop encircling the vessel.
This loop is called the ansa subclavia.
Fibres of the oculosympathetic pathway then rejoin and ascend through the middle cervical ganglion.
These neurons then terminate in the superior cervical ganglion adjacent to the carotid bifurcation(4).
Third order neurons
Post-ganglionic fibres exit the superior cervical ganglion forming a sympathetic plexus.
This enters the carotid canal before dividing into medial and lateral branches of a ‘carotid plexus’.
As the name suggests these bundles of nerve fibres follow the branches of the carotid artery.
The medial branch closely associates with the internal carotid artery within the cavernous sinus.
Branches supply a number of cranial nerves: oculomotor,
trochlear,
ophthalmic division of the trigeminal and abducens.
Fibres also supply the ciliary ganglion within the orbit.
Together these fibres form an intricate sympathetic network innervating the orbit.
Fibres from the lateral branch of the carotid plexus temporarily join the abducens nerve (CN VI).
Almost immediately fibres leave this structure to anastamose with the ophthalmic division of the trigeminal nerve (CN V1).
The pathway then enters the orbit via the superior orbital fissure.
Fibres innervate the eye via long ciliary and short ciliary nerves.
Sympathetic function within the orbit and peri-orbital tissues includes:
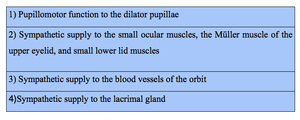
Table 1: Sympathetic function within the orbit and peri-orbital tissues.
As described,
the anatomy of the oculosympathetic chain in its postganglionic portion is complicated.
Ultimately it acts to supply the orbit.
A further post-ganglionic branch of the oculosympathetic pathway follows the course of the external carotid artery.
These clinically relevant sympathetic fibres innervate smooth muscle within blood vessels and sweat glands of the face.
As discussed above,
interruption to these fibres leads to impaired flushing and sweating on the ipsilateral side,
these are typical features of Horner’s syndrome.
Although the anatomical description of central,
pre and postganglionic fibres can aid the radiologist in their search for the site of disruption,
this is not particularly useful clinically.
The site of disease cannot be reliably predicted based on clinical presentation.
Lesions can produce a constellation of neurological signs which may not adhere to the expected anatomical site ( Table 2 ).
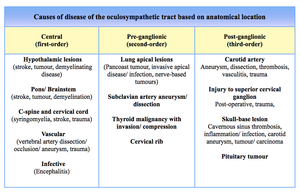
Table 2: Differential diagnoses: disease of the oculosympathetic tract based on anatomical location





