Keywords:
CNS, Neuroradiology brain, MR, MR-Diffusion/Perfusion, Education, AIDS, Infection, Inflammation
Authors:
S. Gerevini, P. cinque; Milan/IT
DOI:
10.26044/ecr2019/C-1295
Aims and objectives
Although HIV replication in the central nervous system (CNS) is generally controlled by systemic combined antiretroviral therapy (cART),
cases of encephalitis associated with cerebrospinal fluid (CSF) viral escape and resembling old HIV-encephalitis (HIV-E) cases of untreated patients are increasingly being observed. Cerebrospinal Fluid (CSF) viral escape,
i.e.,
detectable HIV-RNA in CSF despite undetectable or lower-than-CSF level in plasma,
is seen in approximately 10% of patients receiving combination antiretroviral treatement (cART) [1].
This condition is infrequent,
although individual case descriptions and small case series are increasingly being reported [2-5].
Symptomatic escape seems to originate from continuous,
usually low-grade,
HIV replication in the brain of patients with relatively high CD4+ cell counts.
Indeed,
an inflammatory component may be relevant,
and a pathological entity,
referred to as CD8+ cell encephalitis,
has been reported in patients with symptomatic CSF escape [6].
Although the clinical presentation may be severe,
the outcome is usually good upon cART optimization.
This condition is occasionally associated with neurological problems,
usually consisting of new and progressive cognitive decline and/or focal symptoms and signs,
defining the ‘neuro-symptomatic CSF escape’.
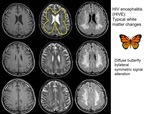
Brain Magnetic Resonance Imaging (MRI) may show diffuse white matter (WM) hyperintensities that recall the presentation of HIV encephalopathy in the pre-cART era.
However,
the frequent finding of CSF pleocytosis and the pathological demonstration of CD8+ T cells brain infiltrates in some cases of symptomatic escape suggest also an inflammatory component.
Indeed,
patients develop symptomatic CSF escape with relatively high CD4+ cell counts and suppressed or low systemic virus replication.
Low nadir CD4+ cells is common,
likely reflecting the establishment of a substantial HIV reservoir in the Central Nervous System (CNS).
In this scenario,
CSF escape seems to result from reactivation of CNS infection when cART potency is lowered,
due to low patient’s adherence,
drug resistance,
or use of drugs combinations that are poorly effective in the CNS,
and cART optimization is key to revert escape and neurological disease in the great majority of cases.
Aim of this study is to analyze the radiological and clinical features of ‘CSF escape encephalitis’ compared to classical pre-cART HIV-E.