
ECR 2019 / C-1295
Brain imaging of CSF HIV escape
Congress:
ECR 2019
Poster Number:
C-1295
Type:
Scientific Exhibit
Keywords:
CNS, Neuroradiology brain, MR, MR-Diffusion/Perfusion, Education, AIDS, Infection, Inflammation
Authors:
S. Gerevini, P. cinque; Milan/IT
DOI:
10.26044/ecr2019/C-1295

Table 1:
TABLE 1: Patients characteristics and laboratory findings at the time of...

Table 2:
TABLE 2: Clinical symptoms and signs are listed here

Table 3:
TABLE 3: MRI findings.
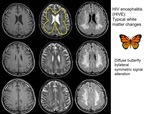
Fig. 1:
HIV encephalitis (HIVE):
Typical white matter changes with relative sparing of...
 and after 10 months (lower line) without therapy")
Fig. 2:
Fig 2: Classic HIV Encefalitis at onset (upper line) and after 10 months (lower...

Fig. 3:
Classic atrophic evolution of HIV encephalitis with enlargement of sulci and...
 or other brain or cerebellum regions associated to a sort of brain swelling (compression on lateral wall of lateral ventricle and effacement of sulci)")
Fig. 4:
Fig 4 A typical case of CSF escape in a patient with standard brain tropism:...
; in some case edema with sulcal effacement can be seen depending of the degree of the underlying atrophy (lower line)")
Fig. 5:
FIG 5: In CSF escape, MRI showed areas of white matter hyperintensity either...
 vasogenic edema is seen as an intense and extensive DWM signal alteration. This edema isn’t associated to DWI changes/ADC restriction due to its extracellular location. This edema can be associated or not with mass effect depending on the degree of edema and underlying atrophy of patient’s brain.")
Fig. 6:
Fig 6 Compared ADC values in healthy controls, classical HIV encephalitis and...

Fig. 7:
Fig 7 Brain MRI during evolution and resolution of CSF escape